Acne represents the most common inflammatory dermatosis seen worldwide and is the leading reason for seeing a dermatologist. This article provides some tips for managing acne in a safe and effective manner to minimize the physical and psychological scars that can result from acne. Tips include how to optimize available treatment regimens according to the evidence base and target therapy to pathophysiologic factors, while also tailoring treatments to patient expectation and needs. Attention is given to minimizing the emergence of antimicrobial resistance in acne patients and beyond.
Key points
- •
Target inflammation early in acne management to avoid scarring.
- •
Consider antibiotic prescribing policies when using antibiotics in the management of acne.
- •
Identify and treat macrocomedones before commencing oral isotretinoin.
- •
Isotretinoin absorption depends on fatty food intake.
- •
Spironolactone may provide an alternative to combined oral contraceptives in female patients who require an antiandrogen therapy.
Introduction
Acne represents the most common inflammatory dermatosis seen worldwide and is the leading reason for seeing a dermatologist. The disease commonly has a prolonged course, with acute or insidious relapse or recurrence over time and associated social and psychological affects that negatively impact on quality of life. Clinical presentation varies and includes open or closed comedones, papules, pustules, or nodules extending over the face and/or trunk. Discomfort may be a significant manifestation of the inflammatory lesions. Seborrhoea is usually present, although the degree may vary. The combined impact of acne frequently results in psychosocial morbidity. Successful treatment correlates with improvement of psychological factors in many. This article provides a top 10 list of clinical pearls to aid the successful management of acne.
Introduction
Acne represents the most common inflammatory dermatosis seen worldwide and is the leading reason for seeing a dermatologist. The disease commonly has a prolonged course, with acute or insidious relapse or recurrence over time and associated social and psychological affects that negatively impact on quality of life. Clinical presentation varies and includes open or closed comedones, papules, pustules, or nodules extending over the face and/or trunk. Discomfort may be a significant manifestation of the inflammatory lesions. Seborrhoea is usually present, although the degree may vary. The combined impact of acne frequently results in psychosocial morbidity. Successful treatment correlates with improvement of psychological factors in many. This article provides a top 10 list of clinical pearls to aid the successful management of acne.
Acne duration and inflammation correlate to the degree of scarring
There is now clear evidence that acne scarring is more likely to occur if treatment is delayed. Recent work presented at the American Academy of Dermatology demonstrated the importance of inflammation in the development of scarring. Both the degree and the duration of clinical inflammation influence resultant scarring.
This emphasizes the need to establish how long the acne has been present when first assessing a patient and to then implement treatment targeting inflammation early in the course of the disease to reduce the likelihood of scarring.
Table 1 outlines an evidence-based algorithm that summarizes treatment options for managing acne. Once under control it is important to consider maintenance therapy with a topical retinoid +/- benzoyl peroxide (BPO). Topical retinoids are the treatment of choice for maintenance therapy because they impact on the microcomedo that represents the precursor of inflammatory and noninflammatory acne lesions.
| Mild | Moderate | Severe | |||
|---|---|---|---|---|---|
| Comedonal | Papular/Pustular | Papular/Pustular | Nodular b | Nodular/Conglobate | |
| First choice | Topical retinoid | Topical retinoid + topical antimicrobial | Oral antibiotic + topical retinoid ± BPO | Oral antibiotic + topical retinoid ± BPO | Oral isotretinoin c |
| Alternatives a | Alt. topical retinoid or Azelaic acid d or Salicylic acid | Alt. topical antimicrobial + alt. topical retinoid or Azelaic acid d | Alt. oral antibiotic + alt. topical retinoid ± BPO | Oral isotretinoin or Alt. oral antibiotic + alt. topical retinoid ± BPO/azelaic d acid | High-dose oral antibiotic + topical retinoid + BPO |
| Alternatives for females | See first choice | See first choice | Oral antiandrogen + topical retinoid/azelaic acid d ± topical antimicrobial | Oral antiandrogen + topical retinoid ± oral antibiotic ± alt. antimicrobial | High-dose oral antiandrogen + topical retinoid ± alt. topical antimicrobial |
| Maintenance therapy | Topical retinoid | Topical retinoid ± BPO | — | — | — |
a Consider physical removal of comedones.
b With small nodules (>0.5–1 cm).
c Second course in case of relapse.
d There was not consensus on this alternative recommendation; however, in some countries azelaic acid prescribing is appropriate practice.
Antibiotic resistance can be associated with reduced clinical response and drives resistance in Propionibacterium acnes and other commensal bacteria: consider antibiotic prescribing policies
There has been a steady rise in antibiotic resistance in Propionibacterium acnes as a result of topical antibiotic formulations used for acne and a heavy reliance on antibiotics in long-term acne management. Resistance in P acnes is significantly more common to erythromycin and clindamycin than to tetracyclines. In the United Kingdom the only community study conducted confirmed that 47% of 649 patients were colonized by erythromycin-resistant propionibacteria and 41% by clindamycin-resistant strains, whereas only 18% were colonized by strains resistant to tetracyclines. Resistance rates in hospital settings globally are much higher.
Once colonized with resistant propionibacteria the resultant effect is most likely to be a reduced response or relapse rather than no response at all. However, studies have clarified that the carriage of antibiotic-resistant strains reduces the efficacy of systemic erythromycin and to a lesser extent oral tetracyclines.
In the United States the prevalence of antibiotic resistance to oral macrolides has rendered them far from useful in the management of acne. The situation as a result of topical antibiotics used in acne is less clear, although a reduction in the efficacy of topical erythromycin over time has been demonstrated in a meta-analysis. Although acne is not infectious, antibiotic-resistant P acnes are transmissible between subjects by person-to-person transfer of pre-existing resistant strains. This can result in an untreated person being colonized with resistant strains potentially making them less susceptible to antibiotic treatment.
Antibiotics may also impact on pathogens other that P acnes . Studies have previously demonstrated profound changes in the resident flora of skin and nonskin sites during antibiotic therapy for acne. Oral antibiotic therapy exposes all body sites with a resident commensal flora to selective pressure. When delivery is topical, selective pressure for the overgrowth of resistant strains and species is largely confined to the skin. Antibiotic-resistant strains of coagulase-negative staphylococci rapidly replace susceptible strains on the skin and in the anterior nares during oral and topical antibiotic therapy for acne.
Increased numbers of coagulase-negative staphylococci resistant to multiple antibiotics have also been found on the skin of untreated contacts of patients with acne managed with sequential antibiotics. Similarly, increased numbers of coliforms, such as Escherichia coli resistant to multiple antibiotics, have been found in the gastrointestinal tracts of patients with acne and their relatives during treatment with oral tetracycline. The judicious use of antibiotics is essential when prescribing for acne and antibiotic prescribing policies are now advocated in the management of acne ( Table 2 ).
| Strategy to Avoid Propionibacterial Resistance Emerging | Comments |
|---|---|
| Avoid inappropriate use of topical and systemic antibiotics | Use oral antibiotics for 3 months in the first instance and only continue if clinical improvement continues |
| If extending the duration of oral antibiotics use combination therapy | Combine with an agent that reduces the likelihood of promoting antibiotic propionibacterial resistance (eg, benzoyl peroxide) |
| If repeated courses of antibiotics are required and the initial clinical response was favorable, reuse the same drug | This avoids multiple resistant strains emerging |
| Avoid prescribing different oral and topical antibiotics concomitantly | This avoids multiple resistant strains emerging |
| Consider using topical retinoids and nonantibiotic antimicrobials wherever possible | These do not promote resistant isolates and when used with antibiotics may achieve more rapid efficacy so reduce the duration of the antibiotic course |
| Topical BPO is fully active against sensitive and resistant strains of P acnes and able to eradicate resistant isolates | BPO can be used for 7 days between antibiotic courses; short contact BPO seems to be more efficacious for clearing P acnes on the trunk than BPO washes |
| Remember to check medical adherence | Poor adherence to antibiotic therapies promotes resistance |
The efficacy of some combined topical therapies rivals that of oral tetracyclines. Prescribing a fixed-dose combination product may also improve adherence and guarantees concomitant use of both drugs. Combination therapy is not usually required for mild acne; BPO or a topical retinoid (tretinoin, isotretinoin, or adapalene) are treatments of choice and are selected according to apparent lesion type, with retinoids being superior in treating comedonal lesions. BPO can be used as a stand-alone treatment for mild papulopustular acne. It is a more potent antibacterial than antibiotics and is highly effective in rapidly reducing propionibacteria whether sensitive or resistant strains are present.
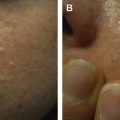
Acute flare of acne on commencing oral isotretinoin: be aware of the macrocomedone
The most common reason for an acute acne flare after commencing oral isotretinoin relates to the presence of macrocomedones ( Fig. 1 ). Macrocomedones may be subtle particularly in the context of significant inflammation. Examination should be done under suitable lighting with the skin stretched. Once identified isotretinoin should be delayed or commenced at a very low dose until macrocomedones have been treated with light cautery or hyfrecation.
If patients still suffer an acne flare at the start of a course of isotretinoin, an antibiotic can be used in combination with oral isotretinoin (eg, erythromycin, 1 g daily, or trimethoprim, 200 to 300 mg twice daily). Tetracyclines should not be combined with isotretinoin because of a possible increased risk of benign intracranial hypertension. If the acne is very inflammatory, then low-dose isotretinoin (0.2–0.4 mg/kg/day) alongside oral steroids (0.5–1.0 mg/kg/day) may be required.
Persistent deep pustules may reflect Staphylococcus aureus in approximately 1% of patients. A bacterial swab should be performed and antistaphylococcal therapy prescribed alongside the oral isotretinoin.
Isotretinoin absorption is food dependent. An empty stomach may reduce absorption leading to a significant reduction in blood levels: ensure patients know how to take isotretinoin because this may impact on safety, efficacy, and duration of therapy
The half-life of isotretinoin is 22 hours. Early studies with oral isotretinoin found that it was 1.5 to 2 times more bioavailable with food ingested 1 hour before, concomitantly with, or 1 hour after dosing than when given during a complete fast. Absorption is markedly affected by the presence of fat and pharmacokinetic studies show that if no food is ingested with isotretinoin the fasting plasma levels of isotretinoin after intake of standard oral formulations can be up to 60% lower than levels obtained in the fed state. This may have a significant impact on efficacy and safety. Isotretinoin capsules should therefore be taken with fatty food at the same time of day. The dose can then be adjusted according to clinical response and presence or absence of side effects.
Posttherapy relapse is said to be minimized by treatment courses that amount to a total of least 120 to 150 mg/kg, with greater than 150 mg/kg not providing a better therapeutic response for acne. The duration of therapy varies according to the dose administered over the course of the treatment period. The range is usually 16 to 30 weeks, and the mean between 16 and 20 weeks, with patients receiving 0.5 mg/kg/day requiring a longer course of therapy to achieve previously recommended cumulative dosing and desired clinical results. Early studies aimed at deriving a cumulative dose for maximum benefit and reduced relapse rate confirmed an effect of dose and duration of therapy but not a pharmacokinetic reason to support the concept of accumulation of drug or a cumulative dose effect. Recent publications suggest that the dose should be tailored to the tolerability of the drug and the clinical response and have demonstrated that the cumulative doses previously recommended may not be necessary in all patients or be achieved if patients are not taking the drug appropriately. There may be significant differences in the absorption of the drug determined by diet in different individuals. Novel formulations less dependent on fatty food for absorption have been developed and are undergoing efficacy and safety assessments, but when prescribing a generic form the importance of ingesting oral isotretinoin with food to maximize bioavailability should be emphasized and the duration of therapy should be adjusted to give at least 90% clearance of acne based on initial clinical acne grade scoring techniques followed by 4 to 8 weeks of consolidation.
Related posts:
 The Relationship of Proper Skin Cleansing to Pathophysiology, Clinical Benefits, and the Concomitant Use of Prescription Topical Therapies in Patients with Acne Vulgaris
Use of Oral Contraceptives for Management of Acne Vulgaris
The Clinical Relevance of Antibiotic Resistance
Evaluation of Acne Scars
Physical Modalities (Devices) in the Management of Acne
The Relationship of Proper Skin Cleansing to Pathophysiology, Clinical Benefits, and the Concomitant Use of Prescription Topical Therapies in Patients with Acne Vulgaris
Use of Oral Contraceptives for Management of Acne Vulgaris
The Clinical Relevance of Antibiotic Resistance
Evaluation of Acne Scars
Physical Modalities (Devices) in the Management of Acne
 When Acne is Not Acne
When Acne is Not Acne
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


