Microsurgical toe-to-hand transplantation remains a valuable reconstructive option for severe, mutilated hand injuries ever since its inception in the 1960s, allowing composite replacement of amputated digits through a single-stage procedure with minimal donor morbidity. Increased experience over the past 40 years has allowed establishment of certain principles that yield consistent results with optimal functional and esthetic outcomes. This article critically examines the latest innovations and refinements in the continual pursuit of excellence for microsurgical toe-to-hand transplantation.
This article attempts to summarize some of these most recent innovations, many of which have been built on previous foundations that had remained surprisingly unchanged over the past four decades. Each section will generally describe what is accepted as current or established practice, examine what is new or controversial and finally offer concluding views on the subject. Ever since the first toe-to-hand procedure, as reported by Nicolandi with the use of a pedicled great toe, the logic of using toes to replace digits was immediately appreciated but not widely practiced until the advent of microsurgery. The first successful microvascular toe-to-hand transplantations were carried out by Yang and Gu and Cobbett using the second toe and great toe, respectively, for thumb reconstruction. Since then, toe-to-hand transplantation has occupied a special role in the history of microsurgery, being among the first few free tissue transfers to be attempted in humans and also as a rich source of innovation and technical refinements for microsurgical procedures in general. The ever-growing wealth of literature bears testament to the increasing acceptance of toe-to-hand transplantation and also the ongoing innovations and refinements in the pursuit of excellence. This article attempts to summarize some of these most recent innovations, which are built on previously established foundations, many that remain surprisingly unchanged over the past 4 decades. Each section will generally describe what is accepted as current or established practice, examine what is currently new or controversial, and finally offer concluding views on the subjects.
Initial assessment and management of the injured hand
Established Practice
Following digital amputations, the replacement of “like-for-like” tissues that can potentially restore the exacting demands of different digits is achievable only by a successful replantation. In cases of nonreplantable or failed replantations, toe-to-hand transplantations remain the next-best option with a far superior result than the use of prosthesis or other nonmicrosurgical techniques. Initial assessment of the injury may prompt a preemptive discussion with the patient regarding the possibility of toe-to-hand transplantations, especially if the success of replantation is in doubt, such as in cases of severely avulsed, crushed, or multiple amputations. Such a preemptive approach provides guidance for the initial management of the injured hand; the surgeon is reminded to maximally preserve all vital structures, such as neurovascular bundles, tendons, bones, joints, and soft tissues, which will greatly facilitate the subsequent toe-to-hand transplantation. Any soft tissue defects can be temporarily covered using an interim groin flap with the following advantages:
- 1.
It avoids the need for excessive shortening of vital structures by providing soft tissue protection.
- 2.
It avoids skin grafts in the hand.
- 3.
It avoids the need to include a large amount of skin with toe harvest, thus facilitating primary closure in the donor site.
- 4.
It avoids the need for local flaps in the hand, which may cause further scarring.
- 5.
It provides redundant skin that can be used for web space reconstruction.
In the highly motivated and well-informed patient, primary toe-to-hand transplantation (before the wound is healed) can be reliably performed without an increased risk of complications or need for secondary revisions.
Immediate, 1-Stage, and Total Reconstruction
Over the past 2 decades, increased experience in microsurgical toe-to-hand transplantation and free tissue transfers in general has led to a move toward immediate or primary, 1-stage, and total reconstruction. An increasing number of immediate toe-to-hand transplantations have recently been described for total thumb or partial thumb defects, reflecting perhaps an increasing comfort with the indications of toe-to-thumb transplantation and its growing establishment as the definitive choice of thumb reconstruction by patients and surgeons alike. Other than minimizing the number of operations, these immediate procedures shorten the rehabilitation period and provide great psychological benefits without compromising the functional or esthetic outcome. For similar reasons, 1-stage reconstructions offer the advantage of earlier return of function and avoid the need for multiple operations. Another recent area of development is the increasing reports for 1-stage reconstruction involving digit amputations with associated soft tissue defects. Although these soft tissue defects can be reliably covered with nonmicrosurgical loco-regional or pedicled flaps or with microsurgical workhorse flaps, the problem is multiplied when toe-to-hand transplantation is also required for replacing missing digits. The amount of soft tissue that can accompany the toe is limited, as is the number of recipient vessels in the hand for multiple microsurgical procedures. Various investigators have recently reported different approaches to tackle these limitations. Fan and colleagues, for example, described the use of a second free flap in conjunction with the toe transplantation to re-create a contracted web space where the accompanying free flap was anastomosed to the donor vessels of the toe via a “chain-link” fashion to present a single unit of anastomosis in the recipient hand. Thomas and Tsai described a case report where a combined second and third toe unit was anastomosed to a reversed radial forearm flap to resurface a dorsal-palmar hand defect with multiple finger amputations. del Pinal and colleagues described a dorsalis pedis fascio-subcutaneous toe free flap to reconstruct the missing digit, as well as overcome medium-size defects in the hand, with little donor morbidity. More recently, Zhang and colleagues reported a series using a triple chimeric flap (including skin from the anterior tibial area, the dorsum of the foot, and a transplanted toe) based on the anterior tibial artery or resurfacing accompanying extensive defects in the hand. The donor defect subsequently required extensive skin grafting of the anterior tibial area and the dorsum of the foot.
A further area that has attracted interest is to achieve total reconstruction in one setting. Other than soft tissue defects, traumatic amputations of digits may be accompanied by component loss of bone, nerve, or tendon. As a logical choice, the foot represents a natural warehouse for replacing different missing components with “like-for-like” tissues. del Pinal and colleagues described the use of neurocutaneous vascularized nerve grafts harvested from the tibial side of the second toe to reconstruct nerve defects of up to 4 cm for important finger contact surfaces (eg, ulnar side of thumb or radial side of index finger). Earlier, they also described the application of 1-stage vascularized toe bone blocks for complex intercalated bone defects in the fingers. From our own institution, a new reconstructive strategy was designed using a combined harvest of the metatarsophalangeal joint and second toe extensor digitorum brevis muscle for simultaneous abductoplasty and joint reconstruction to restore opposition and thumb reconstruction in a single stage.
These recent reports illustrate an increased move toward primary, 1-stage, and total reconstruction of the mutilated hand. Indeed, this reconstructive philosophy has been practiced and developed in our institution since the 1990s, where accumulated experience with adequate debridement followed by immediate or primary toe transplantation, functional reconstruction, and continual refinements where different flaps are tailored for different defects have proven the safety and advantages of these approaches. Some caution is warranted, however, when encountering the mutilated hand with extensive soft tissue defect. The upper extremity poses a reconstructive challenge for the surgeon because of the limitation of recipient vessels. In the traumatic situation, judicious use of available vessels becomes even more critical, as some of these vessels may be damaged. Sacrificing a set of potential recipient vessels for any reconstructive procedures other than toe transplantation should therefore be carefully considered. For similar reasons, sacrificing a major vessel, for example, by performing a reversed radial forearm flap to resurface hand defects in conjunction with a toe-to-hand transplantation should probably be contraindicated. Furthermore, any method to ensure survival of multiple free flaps (including the toe transplantation) on a single set of anastomosis should also be discouraged. In such a “flow-through” design with 2 microsurgical free tissue transfers including the toe transplantation, a single thrombotic event could potentially lead to the loss of both flaps with no chance to salvage either of the flaps.
In principle, whereas we advocate a single-stage reconstruction wherever possible in properly selected cases, a staged reconstruction may sometimes be the best choice to produce the best functional outcome. An example can be seen from our recent series of osteoplastic reconstructions for thumb defects. Of 24 patients who received osteoplastic thumb reconstruction for amputations proximal to the metacarpophalangeal joint, 10 received subsequent toe transplantations as a secondary procedure with the primary osteoplastic reconstruction, avoiding the need for unnecessary toe transplantation in 14 patients who achieved good enough function without further reconstruction. This staged approach was also advantageous in augmenting the length of the remaining stump, thus limiting the length of toe that needed to be harvested and thus reducing donor morbidity. More importantly, it allowed a more strategic positioning of the subsequent transplanted toe by guiding the toe inset into a suitably abducted position as a result of the osteoplastic thumb reconstruction.
Considerations of Donor Site Morbidity
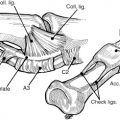
The key objective of any new method is, and always should be, to achieve optimum functional results. The pursuit of this objective should, however, be carefully balanced against the cost of donor site morbidity. Since its first description, the combined dorsalis pedis flap in conjunction with toe transplantation has been a highly appraised option for resurfacing of associated soft tissue loss with digit amputation. The use of skin grafts to resurface the donor foot defect, however, is notorious in creating an unstable surface that is often painful and prone to wound break down. For this reason, primary closure of the donor site should always be achieved to prevent painful scars on the foot and also delays in ambulation. In our experience, the amount of skin to be harvested with the toe is always deliberately restricted. If additional skin is needed for resurfacing accompanying defects in the hand, it should be recruited from sources other than the foot. For this reason, and also for those mentioned previously, the pedicled groin flap is still our preferred option. It obviates the need for a second set of recipient vessels for micro-anastomosis and leaves an almost negligible donor scar. The amount of soft tissue that can be harvested is abundant to cover most defects and to recreate a new web space if necessary. The major drawback remains the inconvenience of a staged procedure and the need for hand attachment to the groin for a few weeks. However, those problems can be easily overcome with careful patient explanation and creative rehabilitation by the physiotherapists ( Fig. 1 ).
Decision making for toe-to-hand transplantations
Established Practice
The decision of whether to proceed with a toe-to-hand transplantation often needs to take into consideration factors “external” to the hand, such as the general condition of the patient, level of surgeon’s microsurgical experience, and also the available resources. Once a decision has been made, the subsequent choice of toe or its variation depends on “internal” factors drawn from examination findings of the injured hand.
Thumb Amputations
The function of the thumb decreases by 50% once the amputation level is proximal to the proximal interphalangeal joint and approaches 100% once it crosses the metacarpophalangeal joint. For this reason, the interphalangeal joint is usually considered the minimum functional length for adequate prehension. Patients who present with an amputation distal to the interphalangeal joint should be considered for toe-to-hand transplantations on a “case-by-case” basis, whereas it should always be offered for amputations proximal to this level. Other factors guiding the choice of toe flap include the functional and cosmetic requirements of the patient, the size of the contralateral normal uninjured thumb, and the condition of the thenar musculature or carpometacarpophalangeal joint. The various options for thumb reconstruction therefore include the total great toe, trimmed great toe, great-toe wrap-around flaps, and the second toe.
Finger Amputations
Factors to consider in finger reconstruction include the level of amputation (proximal or distal) and the number of fingers involved (single or multiple). Perhaps more so than the thumb, finger reconstruction using toe transplantation is guided by the specific occupational or cosmetic needs of the patient. In general, toe transplantations for proximal amputations in a single finger are largely unacceptable because of the suboptimal functional and cosmetic outcomes. Distal finger reconstruction, however, seems to be enjoying increasing popularity with excellent outcomes reported (see later in this article). Multiple proximal finger amputations carry a morbidity approximating that of thumb loss and should always be considered for reconstruction.
Metacarpal Hand
“Metacarpal hand” involves amputations of all fingers proximal to a functional level (middle of the proximal phalanx) with or without the involvement of the thumb. The significance of this injury lies in the loss of basic prehension abilities owing to missing opposable elements. At present, toe-to-hand transplantation represents the only option in these injuries capable of restoring any form of useful prehension. A classification system based on the level of finger amputations (type I) or thumb amputations (type II) has been widely used for the management of this condition ( Fig. 2 ). The different reconstructive options proposed in these 2 classifications offer clear management pathways that take into account not only the level of amputations, but also important factors like the status of the thenar musculature or carpometacarpophalangeal joint.
These established principles greatly facilitate decision making when considering the appropriateness of toe-to-hand transplantation and also the choice of toe flap for reconstruction. Whereas toe-to-hand transplantation was once confined mainly to the reconstruction of total thumb or multiple finger loss, there are now increasing numbers of reports using toe-to-hand transplantations for isolated distal partial thumb or finger defects. Woo and colleagues reported a series of distal thumb reconstructions with different great toe flaps. Similar to our previous description of the great toe modified wrap-around flap, recommendations were made to always include the distal phalanx when harvesting a partial or total great toe to prevent iatrogenic injury to the germinal matrix. For significant volar surfaces, toe pulp transplantations continue to be worthwhile options in providing a sensate, stable pulp surface, especially if the use of local flaps runs the risk of further restricting global hand function. Pulp flaps can be reliably harvested from the fibula side of the great toe, with primary closure of the donor site achievable if the width of the flap is less than 10 to 12 mm. Although the second toe has been proposed for the same purpose, the limited width of flap available means that skin grafting is invariably necessary, which creates significant donor site problems. For dorsal thumb loss or combined dorsal-volar losses, the harvest of a bigger unit from the great toe, including the nail bed, as suggested by Woo and colleagues, should be approached with caution because of the larger donor defects that have to be grafted or closed with cross-toe flaps.
Distal finger reconstruction has also gained popularity in recent years. Another report by Woo and colleagues found great patient satisfaction when using toe transplantation for missing fingers at the distal interphalangeal joint level. This supports our previous concept that toe-to-hand transplantation when performed purely for cosmetic or psychological reasons is justified in properly selected patients. Distal toe transplantation is not only able to replace the original length of the amputated digit, but also reproduce the cosmetic appeal of a nail. In our opinion, distal finger–toe transplantation should be considered a good indication ( Fig. 3 ). In contrast, proximal finger–toe transplantation (proximal to the proximal interphalangeal joint) for isolated finger amputation continues to be an area of difficult decision making, as it is nearly always impossible for the transplanted toe to match the length of the original digit and to resume the same finger cascade. We recommend that proximal finger–toe transplantation for single finger amputation be offered only to patients who are very clear about their goals and who are willing to accept the limitations of a shorter reconstructed finger. Furthermore, it should be offered only for radial digit (index or middle finger) amputations because of the possible functional gain of pulp-to-pulp pinch from these fingers.
Recent work has also been reported for multiple finger amputations. del Pinal proposed the concept of the “balanced” or “acceptable” hand as a guide to decision making for achieving the final aim of a harmonious digital arcade. Strong recommendations are made for reconstruction of central finger losses (the unbalanced hand) or to reconstruct at least 1 of 2 distal finger losses, reinforcing the importance of the tripod pinch, which has previously been reported from our series of multiple finger amputations. Although the number of true metacarpal hand injuries has decreased in number owing to improved standards in industrial safety, interesting points are still being raised in recent reports with regard to classification and management of such injuries. Fan and colleagues attempted to confine the donor defect of a metacarpal hand (type IIA) reconstruction to one foot by harvesting a great toe wrap-around flap and combined second and third toe based on a single arterial pedicle. Kotkansalo and colleagues used different configurations of toe transplantations for metacarpal hand defects with an alternative classification: level A refers to amputations with resultant intact finger metacarpophalangeal joints and thumb amputation distal to the metacarpophalangeal joint; level B refers to amputations proximal to the finger metacarpophalangeal joints and thumb amputations with resultant thenar or carpometacarpophalangeal joint disruption (analogous to Wei’s classification of IIC and IID); level C refers to a transcarpal amputation; and level D refers to a more proximal wrist level or distal antebrachial amputation. This classification is useful in providing information for more proximal or antebrachial amputations where the usefulness of toe-to-hand procedures has been previously demonstrated. However, with experience drawn from a relatively small number of patients, many of their philosophies contrasted sharply with ours for reconstruction of the metacarpal hand. The major differences between this classification and that described by Wei and colleagues is the absence of a clear distinction between different levels of finger amputations (Wei’s type I) and also a separate classification for metacarpal hand defects focusing on thumb reconstruction (Wei’s type II). The reasons for the contrasts are observable from differences in emphasis for thumb and finger reconstruction. For thumb reconstruction, the second toe was preferred in most of this study instead of the great toe. In addition, single-digit pulp-to-pulp pinch was always preferred to the reconstruction of a tripod pinch. These strategies could be based on unwillingness (both patients and surgeons) to sacrifice the great toe for thumb reconstruction and also a reluctance to use a combined second and third toe for finger reconstruction.
For multiple finger amputations, we have been advocating reconstruction of a tripod pinch, wherever possible, for the dominant hand or the unilateral hand injury to achieve increased lateral stability, pinch strength, and width span, where the radial finger provides the main pulp-to-pulp pinch with the thumb, while the additional finger plays the important role of a buttress and stabilizer ( Fig. 4 ). Despite concerns over donor morbidity following combined second and third toe harvest, our experience with more than 200 cases has proved the safety and efficacy of this reconstructive option with an acceptable donor foot morbidity. Our experience with a large volume of thumb reconstruction has also convinced us that the great toe (total or trimmed) is the ideal and superior choice over the second toe. Despite concerns from Kotkansalo and colleagues and others regarding the donor morbidity of losing the great toe, the donor morbidity is generally acceptable if at least 1 cm of the proximal phalanx of the great toe is preserved to protect the integrity of the foot and the windlass mechanism (tightening of the plantar fascia) to enable better push-off and foot stability during both the stance and swing phases of walking. For defects involving the first thumb metacarpal where a longer length of bone is needed, we prefer to use a bone block or a staged reconstruction with an initial osteoplastic ray reconstruction, as described previously. In addition, the left foot is always chosen because of its less dominant role in walking, running, or sport activities. By carefully choosing the donor toes and observing certain surgical principles (see the following section), foot function is well maintained even after the harvest of up to 5 toes, as is necessary for bilateral injuries.