Introduction
It is thanks to the illustrious Austrian surgeon, Carl Nicoladoni that the foot began to be considered as a precious warehouse for all requirements of thumb and digital reconstruction. In his three papers (1897, 1900, 1903), he described the use of pedicled toe transplantation as a valid option for reconstruction of missing digits, rather than sacrificing viable tissue in an already injured hand. The obvious inconvenience of attaching the hand to the foot for several weeks limited the popularity of this technique. Between the 1960s and 1970s, encouraged by the advent of the microsurgical era, brilliant surgeons such as Harry Buncke, Yang Dongyue, and John Cobbett illustrated experimentally, and applied clinically, the first microsurgical toe transplantations. Subsequently, the functional and aesthetic innovations by Morrison with the wrap-around toe, Wei with the trimmed great toe transfer, and many others rendered this procedure a safe and reliable first choice in the reconstructive ladder of hand trauma.
Flap Anatomy (see Figure 54.1 , Fig 13.7 , Fig 13.8 , Fig 13.11 , Fig 13.15 , Fig 13.17 , Fig 13.19 )
The metatarsophalangeal (MTP) joint of the great and lesser toes has a wider range of motion in extension than flexion. The interphalangeal (IP) joint of the great toe allows a slight extension of about 12° and a wider flexion of about 46°, whereas the proximal and distal interphalangeal joints of the lesser toes do not allow for any extension.
The principal function of the toes has been described as the capacity to oppose efficiently against the ground reaction force in the late stance phase of the gait cycle. In this part of the gait cycle, in fact, the metatarsophalangeal joints of the toes are passively led to 70–90° of dorsiflexion, as a consequence of the forward progression of the body while walking. The toes oppose such movement by means of a passive and active mechanism. The former is related to the plantar aponeurosis and the latter to the extrinsic and intrinsic musculature. The plantar aponeurosis extends from the os calcis to the base of the first phalanx of the toes, as well as the sesamoid bones. Its main function is related to the windlass effect mostly present under the first and second metatarsal rays, where this fibrous band guarantees the maintenance of the medial longitudinal arch of the foot. The intrinsic musculature inserts on the base of the first phalanx of the toes and, in the great toe, on the sesamoid bones. They participate in providing a good foothold by active pressure against the ground. The extrinsic musculature of the toes is represented by the flexor and extensor hallucis longus and flexor and extensor digitorum longus of the lesser toes. These muscles work in synergy with both ankle plantar- and dorsiflexors, balancing the forward progression of the tibia, especially in running and jogging.
Harvesting of the great or lesser toes implies the interruption of one or more of these anatomic structures, which can lead to flattening of the foot, modification of the pressure distribution beneath the foot during the gait, and consequent callus formation under the remaining metatarsal heads.
Arterial Supply of the Flap (see Figure 54.1 , Fig 13.7 , Fig 13.15 , Fig 13.17 )
Toe transfer can be based on the dorsal arterial system, mainly provided by the dorsalis pedis artery and its terminal branches, or on the plantar arterial system formed by the plantar metatarsal arteries.
Great Toe, Second Toe, and Combined Second and Third Toe Flaps
Dominant:
first dorsal metatarsal artery (FDMA)
Length: 5 cm (range 4–6 cm)
Diameter: 1.3 mm (range 0.6–2.4 mm)
In about 70% of cases, the FDMA is bigger than the first plantar metatarsal artery (FPMA). The dissection of the FDMA, whether lying superficial or in the context of the interosseous muscle, is usually straightforward. An increased vascular diameter can be obtained by proceeding directly into the larger dorsalis pedis artery.
The proper plantar digital arteries are the effective blood source to the great toe, second toe, and combined second and third toe transfer. Their origin is the distal perforating artery, which connects the FDMA and FPMA distally.
Minor:
first plantar metatarsal artery (FPMA)
Length: 5 cm (range 4–6 cm)
Diameter: 1.5 mm (range 0.6–3.0 mm)
If the FDMA is absent, or of a small caliber, the FPMA is the second choice. Because of its course in the deep compartments of the foot, the dissection usually proceeds until the midshaft of the first metatarsal bone. If necessary, an increased length can be obtained by vein graft. In about 20% of cases this artery is dissected as a dominant vascular source since the FDMA is absent or of inadequate caliber. Despite the dominance of the FDMA or the FPMA, the plantar proper digital arteries are the effective vascular source for great toe, second toe, and combined second and third toe transfers. In 10% of cases, the FDMA and FPMA have a similar diameter, in which case the former is used as a dominant pedicle since it is easier to dissect.
Isolated Third Toe, Combined Third and Fourth Toe Flaps
Dominant:
second plantar metatarsal artery
The dorsal metatarsal arteries arise in 86% of cases from the arcuate artery, which is a lateral branch of the dorsalis pedis artery. The arcuate artery is absent in more than 40% of cases. Its absence does not preclude the transfer.
Minor:
second dorsal and third plantar or dorsal metatarsal arteries
The vessel is selected according to the intraoperative findings and the surgical plan.
Venous Drainage of the Flap (see Fig. 13.19 )
Primary:
the dorsal superficial venous arch and its medial continuation into the great saphenous vein represent the primary venous drainage in most variations of toe flaps.
Secondary:
venae comitantes of the FDMA and FPMA present a much smaller caliber than the great saphenous vein and they are rarely employed.
Nonetheless, they offer a valuable alternative in the postoperative treatment of venous engorgement.
Flap Innervation (see Figure 54.1 , Fig 13.8 , Fig 13.11 , Fig 13.15 , Fig 13.19 )
Sensory:
plantar digital nerves are of fundamental importance in the recovery of pulp sensation.
They must be harvested in great toe, second toe, isolated third toe, and combined second and third, and third and fourth toe transfers. Branches of the superficial peroneal nerve are included in combined toe transfer and isolated third toe transfer. In great and second toe transfers, these branches are not necessarily included since the first web space is supplied mainly by the deep peroneal nerve.
The deep peroneal nerve is distributed to the first web space. Either the medial or lateral branch should always be included in great toe (both trimmed and wrap-around) and second toe transfers.
Even in the absence of valuable sensory branches of the radial nerve in the recipient hand, we still include the dorsal sensory branches from the donor foot and coapt them to the proper digital nerves available in the donor finger.
Flap Components
A wide variety of combinations give the opportunity to plan a custom-made transfer that best adapts to specific situations. The most utilized flaps are the great toe, which allows the whole great toe transfers, the trimmed toe technique, and the wrap-around technique; the second toe, which allows the whole or extended second toe transfers, the wrap-around second toe, and vascularized joint transfers from either the metatarsophalangeal or proximal interphalangeal joint; the third toe transfer; combined second–third and third–fourth toe transfers; and the neurosensory free flaps, which include pulp transfer and first web flap. These flaps are composed of one or all tissues involved, including bone, skin, tendon, joints, nerves, and fat.
Preoperative Preparation
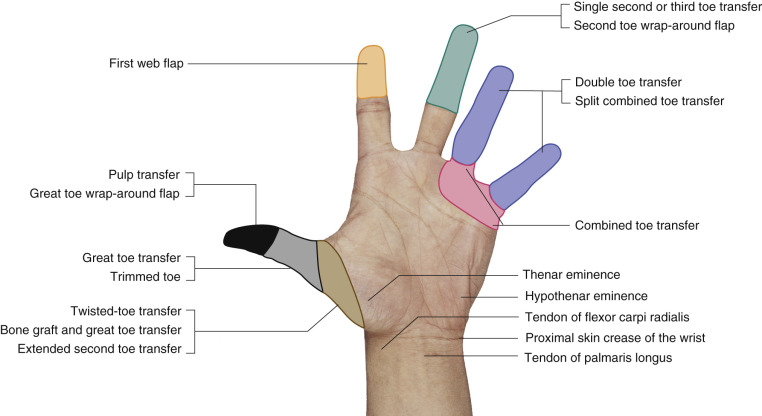
Several possibilities have been developed over the years, with many different kinds of toe flaps available. Appropriate indication is mandatory in order to achieve the best results in terms of function and cosmesis. In Figure 54.2 , some guidelines are presented.
Besides the conventional care given to patients undergoing microsurgical procedures, below are some critical points relevant to candidates for toe transfer.
Age
Toe-to-hand transplantation can be safely performed in patients as young as 1 year old. Young children have a surprising capability of accepting and incorporating a new finger better than adults. Patients as old as 60 years, and nonsmokers who have optimal general conditions, can safely undergo such procedures but the low chance of nerve regeneration and the probability of atherosclerotic change in the arterial tree represent risk factors for failure.
Vascular Pattern
Doppler examination is a useful tool in localizing the presence and position of the dorsalis pedis artery. The FDMA and FPMA can be evaluated with the same method, but not much information is provided related to their exact course in the context of the interosseous muscles. Angiographic assessment of the vascular tree of the foot is not routinely necessary, unless congenital pathologies, previous traumas, or arteriosclerosis would suggest a likely unreliability of the arterial system. Direct visualization of the arterial system by retrograde dissection from the first web space is an invaluable method to appreciate the exact vascular pattern, whether dorsal or plantar dominant.
Recipient Site
In trauma cases, the loss of tissue is preferably covered before the transfer by a pedicled groin flap or free flap. Local flaps should be avoided in order to spare tissue from a hand already traumatized. Plastic models, particularly in proximal thumb reconstruction, can be of great help in order to assess the best length to be harvested and the location that would yield the best outcome and the greatest functional use for the patient ( Fig. 54.3 ). Tinel’s sign facilitates the localization of recipient nerve stumps that, particularly in avulsion amputation, might be unpredictable.

Donor Site
Some authors have stressed the importance of strict control of the temperature in the donor foot before the transfer, noticing that values <32°C may predispose to vasospasm. Dimensions of the defect and the exact size of the toe(s) have to be carefully examined in order to select the appropriate transfer. Discrepancies in the appearance of fingers and toes can be corrected in thumb reconstruction by a trimmed toe or wrap-around technique, as well as a second toe wrap-around flap indicated in avulsion injuries of the fingers. Fungal infections in the toes do not constitute a contraindication to toe transfer since it has been noticed that modification of the local environment leads to a spontaneous resolution of the infection itself.
Anesthetic Considerations
All patients in our department undergo general anesthesia. In addition, axillary plexus blockade is used both intra- and postoperatively for prevention of pain and vasospasm by providing sympathectomy and induction of continuous analgesia. Other centers use epidural and brachial plexus blocks rather than general anesthesia.
Patient Positioning
The patient is placed supine on the operating table with a tourniquet on the proximal thigh. The flap can be harvested with the hip in a neutral position and the knee in full extension. The operator sits beside the operating table facing the dorsal aspect of the foot, while the assistant divaricates the web space depending on the transfer. For the plantar dissection the operator changes position and faces the plantar surface of the foot.
Great Toe Transfer
See Case 54.3 .
Indications
- •
The best results are obtained for amputations through the first phalanx of the thumb. In such cases, the mobility of all three joints of the first ray is restored (see Case 54.3 ).
- •
Amputations at or proximal to the MCP joint with preservation of the thenar musculature can still achieve excellent results, but might necessitate the use of a conventional bone graft in order to restore adequate length to the transfer. In case of loss of the thenar muscles, we perform primary opponensplasty during the transfer. Amputations at the base of the first metacarpal or involving the carpometacarpal (CMC) joint of the thumb require a different approach by either an extended second toe transfer or pollicization.
Advantages
- •
In thumb reconstruction, the great toe provides a wider pulpar and nail surface than the lesser toes, conferring excellent restoration of pinch and grasp power.
- •
Wide range of motion of the metatarsophalangeal joint ( Fig. 54.4 ) if needed; however, removing this joint will increase morbidity at the donor site.
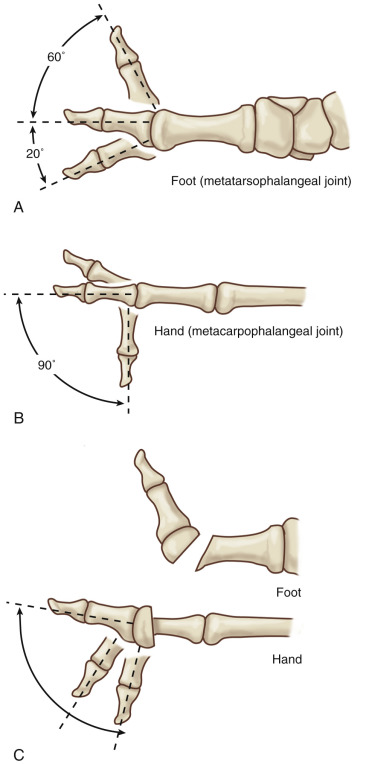
Figure 54.4
(A,B) The metatarsophalangeal joint of the great toe has a wide range of motion in extension; on the contrary, the metacarpophalangeal joint of the thumb moves mostly in flexion. (C) Oblique osteotomy of the first metatarsal avoids hyperextension of the metatarsophalangeal joint of the transferred great toe.
Disadvantages
- •
The cosmetic appearance of the foot is often considered disabling by the patient.
- •
Even though 1 cm of the proximal phalanx of the first ray is usually left in situ, patients may notice a decrease in push-off and manifest different degrees of impairment in running or walking on unstable terrain.
- •
Circumferential diameter and nail width are often clearly bigger than those of the thumb, making the aesthetic result less pleasant.
Flap Design
Soft tissue deficiency at the recipient site should be managed in advance by either a pedicled groin flap or a free flap, limiting the dimensions of skin flaps from the donor foot. Regardless of the level of thumb amputation, we routinely perform an osteotomy of the great toe, preserving 1 cm of the base of the first phalanx. If more length is required, a conventional bone graft is harvested from the hip. The length of the necessary vessels, nerves, and tendons is indicated while exploring the recipient site, so that unnecessary dissection of the foot is avoided.
Anatomic Landmarks ( Fig. 54.5 )
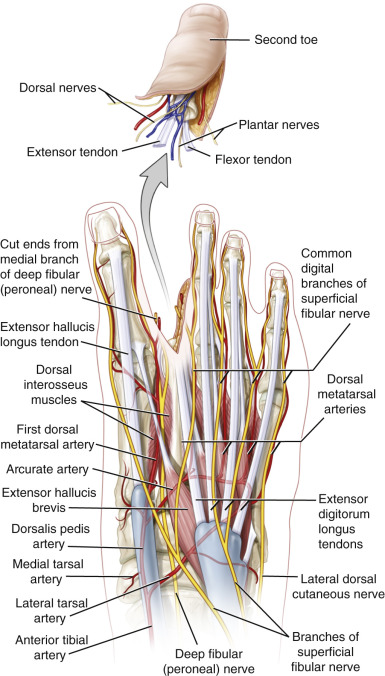
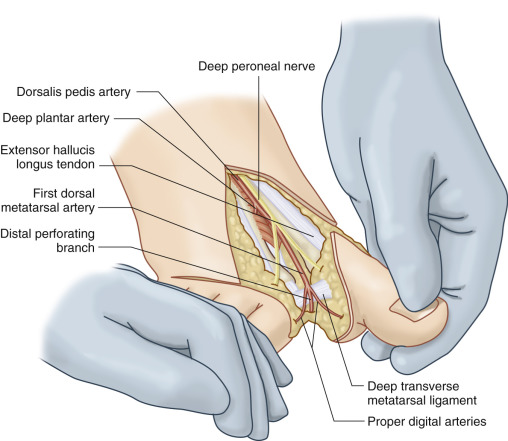
The metatarsophalangeal and interphalangeal joints of the great toe are identified and outlined with a marking pen. By dangling the leg, the superficial venous system becomes visible and the transverse dorsal arch and proximal communication with the great saphenous vein are marked. The dorsalis pedis artery is also marked. If difficulty occurs in visualizing the venous system, a venous tourniquet may be inflated. The extensor hallucis longus, the underlying first metatarsal, and the second metatarsal are identified along their entire course. The artery runs between the first and second metatarsal bones and lateral to the extensor hallucis longus tendon. A line connecting the palpable dorsalis pedis artery to the midpoint of the web space marks the axis of the artery. The terminal branches of the superficial peroneal nerve run subcutaneously along the corresponding intermetatarsal space, parallel to the long extensor tendons. The deep peroneal nerve is located medial to the dorsalis pedis artery. In the midfoot, it courses between the extensor hallucis longus, which lies medial, and the inner part of the extensor hallucis brevis, which lies lateral. In the forefoot, the deep peroneal nerve, crossed by the medial portion of the extensor hallucis brevis, pierces the deep fascia and becomes superficial, running between the extensor hallucis brevis tendon laterally, and the long extensor of the second toe medially.
General Thoughts About Flap Design
A wide skin flap on the first web space or on the dorsal surface of the foot might be considered, but the increase in donor site morbidity makes this extension undesirable. The osteotomy can be planned at the base of the first phalanx, at or proximal to the metatarsophalangeal joint. Routinely, we preserve the base of the first phalanx in order to maintain the distal insertion of the plantar aponeurosis and part of the intrinsic musculature, so preserving the windlass mechanism and the stability of the medial longitudinal arch of the foot. If osteotomy at the metatarsophalangeal joint is planned, it should be performed oblique, dorsal-proximal to volar-distal, for two purposes:
- 1.
Preservation of part of the head of the first phalanx, so that the distal insertion of the intrinsic musculature as well as the sesamoid-phalangeal ligaments can be reattached to the distal stump of the first metatarsal, limiting instability of the medial longitudinal arch.
- 2.
Since the metatarsophalangeal joint has a wider range of motion in extension than flexion, prevention of hyperextension of the transferred great toe will be achieved by pinning the new metacarpophalangeal joint in neutral position ( Fig. 54.4 ).
Special Considerations
As a general rule, the donor site is selected so as to best favor the position of the vascular anastomosis. In thumb reconstruction, the position of the pedicle and the slight lateral angulation of the interphalangeal joint make the ipsilateral great toe the first choice. At the same time, the left great toe can be considered a better option, particularly since drivers might prefer to spare the right foot. Crossing over the tendons by a vascular pedicle of adequate length is a valuable option that does not compromise the blood supply to the toe.
Difference in Design, If Any, When Performing the Flap as Pedicled or Free
A pedicled great toe flap may be used only in areas that lack microsurgical facilities. The design of the flap is similar but a longer vascular pedicle is dissected proximally in order to facilitate transposition to the recipient site.
Flap Dimensions
Generally, the great toe is slightly longer than the thumb and its overall circumference wider, as the width of its nail. As mentioned above, the great toe flap can be harvested distal, at or proximal to the metatarsophalangeal joint. The former is our preferred choice. The skin territory can be limited to a small V-shaped flap on the dorsal and volar surfaces of the foot, or can include the whole first web space and a wide skin flap such as the dorsalis pedis flap.
Flap Markings ( Fig. 54.5A,B )
The midpoint between the great and second toe is marked at the first web space. Medially, a point in line with the osteotomy site is marked and a V-shaped flap is drawn proximally on the dorsal surface of the foot. The length of the V-shaped flap ranges usually between 0.5 and 1.5 cm, allowing primary closure of the donor site. A wider skin flap with the inclusion of either the first web space or the dorsalis pedis flap can be harvested with the great toe, but increased donor site morbidity must be taken into account. A similar V-shaped flap is marked on the plantar surface with its proximal apex slightly shifted between the first and second metatarsal heads in order to avoid any scar beneath the weightbearing areas.
Technique of Flap Harvest
A similar sequence in procedure can be applied to all kinds of toe transfers. The dissection is performed under tourniquet control avoiding the use of an Esmarch band.
Dorsal Dissection
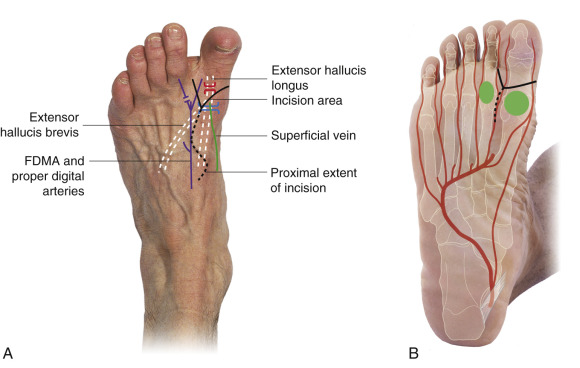
A V-shaped flap on the dorsum of the foot is elevated while taking care to preserve the superficial venous system. The incision starts from the midpoint between the first and second toes. At the first web space, all the soft tissues are carefully excised in order to obtain a clear vision of the dominant arterial system ( Fig. 54.6 ). If the first dorsal metatarsal artery has a greater or equal caliber compared with the first plantar metatarsal artery, the dissection proceeds dorsally in a retrograde fashion, prolonging the skin incision proximally in a lazy S up to the dorsalis pedis artery. Once the dominant arterial pattern has been assessed, a superficial vein of adequate caliber is selected and followed proximally through the dorsal venous arch up to the great saphenous vein on the medial surface of the midfoot. At this level, the dissection is concentrated on the vein, avoiding excessive thinning of the skin, which may lead to skin necrosis of that area. Once the vein has been isolated for the necessary length, the extensor hallucis longus is identified, dissected, and divided at the required length. Branches of the superficial peroneal nerve can be clearly visible during this step and spared.
Now that the superficial venous system and the extensor hallucis longus have been prepared, the dissection proceeds from the first web space distal to proximal in a retrograde fashion in order to isolate the FDMA previously identified. Collateral branches are ligated and the dissection proceeds proximally up to the dorsalis pedis artery, depending on the length needed. The deep peroneal nerve is usually identified while dissecting the FDMA in the forefoot. Its medial branch to the lateral surface of the great toe is followed up to 5–7 cm and divided by intraneural dissection so as to save the lateral branch to the medial surface of the second toe.
If the plantar system is dominant, there is no need for deep dorsal dissection and the artery is followed plantarly in a retrograde manner.
Plantar Dissection
A triangular flap of 0.5–4 cm in height, with the base in the web space, is raised. If the arterial plantar system is dominant, the first plantar metatarsal artery is dissected in a retrograde fashion to the middle portion of the metatarsal shaft. Further dissection might be too disruptive to the foot and the use of a vein graft is advised if a longer pedicle length is required. Most of the fatty pad under the skin is excised and the proper digital nerves on both sides are isolated and harvested as long as needed. Intrafascicular dissection of the first common digital nerve enables the neural fascicles of the second toe to be saved. The flexor hallucis longus is dissected out from its sheath, pulled out, and cut at a proper length. Rarely an additional transverse incision under the medial plantar arch of the foot is needed in order to harvest a longer tendon. After elevating the tendons and the proper digital nerves, the artery and vein are protected, and the soft tissue and the periosteum surrounding the osteotomy site are gently elevated so that the toe can be autonomized by osteotomy, preserving 1 cm of the proximal phalanx ( Fig. 54.7 ). Warm wet dressings are placed over and around the flap and the tourniquet is released. The toe is reperfused for at least 20 min before transfer.
Trimmed Great Toe Transfer ( Fig. 54.8 )
Indications
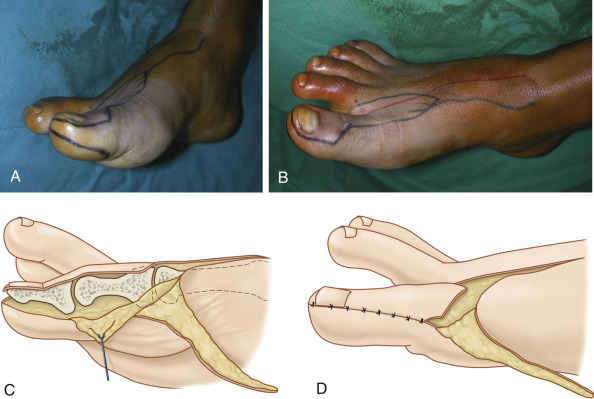
Described by Wei et al. in 1988, the trimmed great toe was conceived for the purpose of improving the discrepancy in the appearance between the great toe and the thumb. Indications are similar to those of great toe transfer when the great toe shows overall dimensions that are evidently bigger than the thumb. Performed in children, the trimmed great toe transfer does not interfere with physiologic growth of the toe.
Advantages
- •
Besides the inherent advantages of great toe transplantation, trimmed great toe transfer offers the best aesthetic match for thumb restoration.
Disadvantages
- •
Disadvantages are similar to those mentioned for the great toe transfer. A slight reduction in mobility of the interphalangeal joint motion is usually observed with the trimmed great toe.
Flap Design ( Fig. 54.8 )
The diameter of the contralateral intact thumb is measured at three levels: the nail eponychium; the interphalangeal joint; and the middle of the first phalanx. The width of the nail is measured as well. The values obtained are marked on the nondominant great toe, so as to create a medial skin flap, tapered on the tip of the toe. This represents the excess tissue, which usually measures 0.8–1.5 mm and is left in situ to allow free tension closure of the donor foot.
Anatomic Landmarks
General Thoughts About Flap Design
The medial skin flap is preserved in order to provide adequate coverage for the remaining portion of the great toe. The dorsal and plantar incisions on the foot reflect the same principles of great toe transfer.
Special Considerations
Accurate reattachment of the medial collateral ligament and capsule of the interphalangeal joint of the great toe avoids instability of the joint itself.
Flap Dimensions
See Great Toe Transfer.
Flap Markings ( Fig. 54.8 )
V-shaped skin flaps are designed on the dorsal and plantar surface of the first ray as shown for great toe transfer. The diameter of the intact thumb is reproduced on the medial surface of the great toe at three levels: the nail eponychium, the interphalangeal joint, and the middle of the first phalanx. The discrepancy in circumference delineates a medial flap that is being tapered at the tip of the toe.
Technique of Flap Harvest ( Fig. 54.8 )
Dissection of vessels, nerves, and tendons is carried out as already described for the whole great toe. The medial skin flap is raised from distal to proximal and the dissection deepened to the bone. A hemi-circumferential joint flap composed of the periosteum, the medial collateral ligament, and capsule is elevated in a dorsal to plantar fashion. By means of an oscillating saw, a longitudinal osteotomy removes 4–6 mm at the joint and 2–4 mm at the proximal and distal phalangeal shaft. After removing the excess tissue, the joint capsule and the collateral ligament are repositioned, taking care to tighten sufficiently to avoid instability of the interphalangeal joint.
Wrap-Around Technique ( Fig. 54.9 )
In the original description by Morrison in 1980, the wrap-around flap was harvested by degloving the great toe, respecting the dimension of the thumb. The soft tissue obtained is used to cover a conventional bone graft that provides stable support. Due to the frequent bone graft resorption and the instability of the pulp, the original technique has been modified in order to include part of the distal phalanx in the flap. This avoids swiveling of the pulp and beaking of the nail, and prevents bone resorption by a higher vascular support either proximal or distal to the conventional bone graft.
Indications
- •
Degloving injuries distal to the metacarpophalangeal joint with skeleton and tendons intact
- •
Complete amputations at the first phalanx of the thumb. In this case a longer bone graft is required, which needs to be shaped in slight flexion at the IP level
- •
This flap is not indicated in children because of the lack of growth capacity.
Advantages
- •
The wrap-around flap produces an optimal aesthetic and functional restoration of the thumb, with minimal loss in length of the great toe.
Disadvantages
- •
The wrap-around flap does not restore joint mobility; therefore, for complete amputations between the MP and IP joints, great toe or trimmed toe transfers are more appropriate.
- •
When part of the distal phalanx is not included, bone resorption, beaking of the nail, and instability of the pulp can be troublesome for the patient.
- •
The bone graft can fracture if overstressed in the first 6 months, and patients should be advised to avoid trauma of the new thumb during that period.
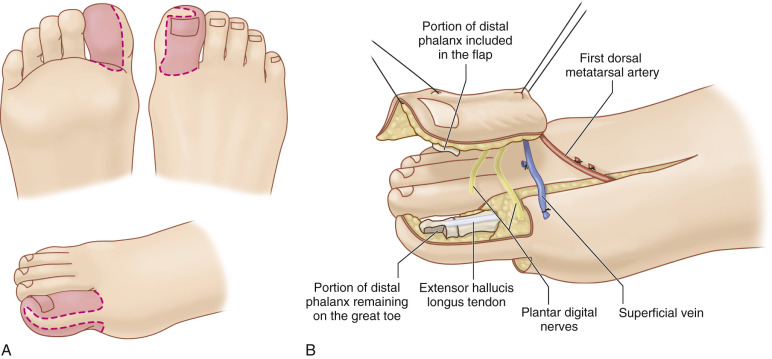
Technique of Flap Harvest ( Fig. 54.9 )
Circumferential measurements of the intact thumb as well as of the nail are traced on the nondominant great toe. A longitudinal skin flap will result on the medial side of the toe, which will taper to the tip of the distal phalanx ( Fig. 54.9A ). The soft tissues are raised off in an avascular plane above the tendon sheath in a medial to lateral direction. During the plantar dissection both plantar digital nerves are identified and included in the transplant ( Fig. 54.9B ). Osteotomy of the distal phalanx can be carried out either transversely, as our preferred choice, or, as described by Doi, longitudinally, elevating the nail with the underlying periosteum and the dorsal cortex as a unique block, preserving the plantar cortex at the donor site. In either case a conventional bone graft is harvested and appropriately shaped depending on the type of osteotomy performed. In Doi’s method the graft will have a flat shape in order to replace the volar cortex of the distal phalanx of the new thumb. The donor site is closed by the remaining medial skin flap and a second cross-toe flap. We usually cover the dorsal defect by a conventional skin graft. Others have suggested the use of a lateral forearm free flap, reverse anterior tibial artery flap, or free peroneal flap.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


