Thumb reconstruction aims to restore the cardinal thumb traits and actions including mobility, stability, sensibility, length, and appearance. The level of thumb loss is divided into thirds: distal (tip to interphalangeal [IP] joint), middle (IP joint to metacarpal neck), and proximal (metacarpal neck to carpometacarpal joint). Distal third reconstruction usually requires only soft tissue restoration. Many options exist for middle third reconstruction, including increasing thumb ray length (metacarpal lengthening, osteoplastic reconstruction, toe transfer) and increasing relative length (phalangization). Proximal third reconstruction is best accomplished with toe transfer, pollicization, or on-top plasty (pollicization of a damaged index finger).
When thumb loss occurs because of trauma, replantation is the best method of reconstruction for most patients. When replantation is not possible, thumb reconstruction is necessary. The level of thumb amputation guides the type of reconstruction, and the level is based on physical examination and radiographic results. The reconstruction should be tailored to the patient’s personal and professional needs. Because significant rehabilitation may be required, the patient must be a willing participant in the reconstruction and rehabilitation.
Functional compensation after distal third thumb loss is easily achieved; therefore, reconstruction at this level typically involves soft tissue only. Techniques such as the neurovascular advancement (Moberg) flap and the cross-finger flap reconstruction are reliable methods for reconstruction at this level. For losses in the middle third of the thumb, restoration of length is a priority. This priority can be addressed via absolute length restoration with metacarpal lengthening, osteoplastic reconstruction, or toe transfer; or via relative length restoration using phalangization of the thumb. Proximal third thumb losses are best treated with microsurgical reconstruction. However, in some cases, microsurgical reconstruction may not be possible. In these situations, transfer of another finger can provide an excellent thumb replacement. A normal finger (typically the index) can be pollicized to become a thumb. A damaged index finger can also be transferred (on-top plasty) to become a stable post for opposition, pinch, and grip.
Hand rehabilitation after reconstruction is absolutely necessary, especially after middle and proximal third reconstructions. Rehabilitation can last for months, and, for some procedures, such as neurovascular island flap reconstruction and digit transfer, sensory reeducation is an important part of the rehabilitation.
By far, the most common cause necessitating thumb reconstruction is trauma. Within the larger trauma classification, thumb injury can be the result of a variety of mechanisms, which include sharp cut, avulsion, and crush. There are some mechanisms that have characteristics of more than 1 injury type. This phenomenon is best illustrated by saw and lawn mower injuries, which have both cutting and crushing components, resulting in a larger zone of injury.
Other insults that can result in thumb loss requiring reconstruction include infections and neoplasms. Thumb reconstruction planning for tumor can be more deliberate than traumatic reconstruction and can often be performed at the time of tumor extirpation.
Because there are many ways to reconstruct a deficient thumb, patients must be educated about the various options so that they may make an informed decision as to which type of reconstruction will serve them best in both the personal and professional settings. In addition to patient input regarding reconstructive methods, the patient must also commit to the reconstructive process and must be a good candidate medically, socially, and psychologically.
In many patients, thumb injuries occur in the workplace, and these patients are affected by the injury because their work requires significant hand use. In these patients, it is essential to work toward a thumb that has adequate length for both gripping and pinching, is stable during activities, has reasonable motion, and is sensate to give tactile input during these actions and to prevent recurrent ulceration or injury. However, adequate length, stability, motion, and sensibility are the end goals for any patient requiring thumb reconstruction, regardless of profession or vocation.
The most important factor in patient selection is the amount and nature of tissue loss that must be reconstructed. The level of amputation is the easiest way to classify thumb deficiencies and is listed in thirds. The distal third extends from the interphalangeal (IP) joint to the thumb tip. The middle third is the portion between IP joint and the metacarpal neck, and the proximal third is from the metacarpal neck to the carpometacarpal joint. Each amputation level presents unique challenges for the patient and the physician, and each level can be reconstructed with multiple modalities.
Treatment options based on injury zone
Distal Third Thumb
Thumb distal third amputations rarely require restoration of length because a thumb amputated through the IP joint remains functional. Therefore, the chief goals of thumb tip reconstruction are soft tissue coverage of bone and length preservation. When there is no bone exposed at the tip of the thumb, closure can be achieved with either healing by secondary intention or skin grafting. Secondary healing of tip amputations up to 1.5 cm diameter with no exposed bone has been shown to result in good 2-point discrimination and is therefore a fairly easy method of achieving coverage. Secondary healing by wound contraction has the advantage of bringing stable sensate skin together to close the defect, as opposed to skin grafts, which can remain insensate. Daily washing and dressing changes with nonadherent gauze are relatively easy for patients. Larger defects with a stable base, however, require skin grafting. Full-thickness grafts are usually preferred because they are more durable and stable, especially in the contact areas subject to pressure and shear. Small full-thickness skin grafts can be harvested from the hypothenar eminence or the volar wrist crease, whereas larger grafts are easily harvested from the groin crease.
When phalangeal bone is exposed at the thumb tip, vascularized coverage is required to preserve length, and there are several flaps that can accomplish this. The main criteria for flap selection are defect size and location of soft tissue loss, specifically if it is volar, dorsal, or at the tip. The Atasoy V-Y advancement flap provides good coverage of the tip of the distal phalanx when only a very small amount of bone is exposed. The technique involves incising the volar pulp of the thumb in a V shape. Scissors are then used to carefully spread the subcutaneous tissue. The subcutaneous attachments deep to the flap, which provide the neurovascular supply to the flap, are left intact. The flap is then advanced distally to close the defect, and the proximal aspect of the V incision is closed side to side, thereby creating the Y shape of the final scar. In practice, this flap is useful for only small defects because of the limited advancement that is possible.
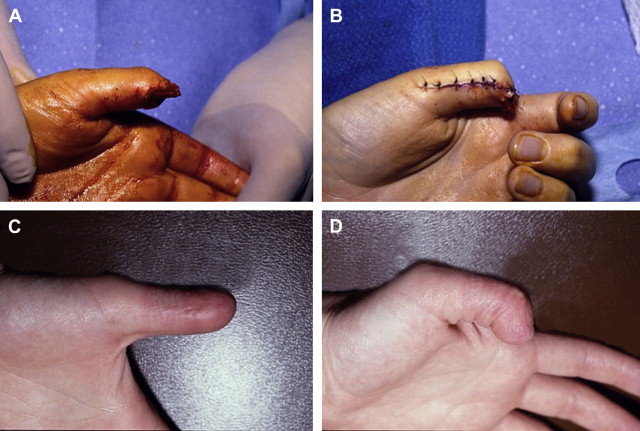
The Moberg or neurovascular volar advancement flap is well suited to cover volar and tip defects of the thumb. It is described as an advancement flap, but the amount of advancement achieved with the conventional rectangular Moberg flap is limited ( Fig. 1 ). Instead, elevation of the flap combined with flexion of the IP joint of the thumb allows the flap to appear to advance distally. To elevate the flap, the midlateral lines are incised on either side of the thumb down to the base of the proximal phalanx. The flap is then elevated from the deeper tissues (flexor sheath) with sharp dissection. The flap includes both neurovascular bundles and all the subcutaneous tissue down to the flexor tendon sheath. The IP joint is flexed, and the flap is inset at the tip. If necessary, a Kirschner wire can be placed across the IP joint to stabilize it. This flap can cover a defect of 1 to 2 cm 2 . A variation of the Moberg flap is the island flap that is incised transversely across the proximal base, and the only remaining attachments are the 2 neurovascular bundles. Unlike the conventional Moberg flap, this method allows a small amount of actual advancement, thereby covering more distal defects. The proximal gap at the base of the flap requires a small skin graft.
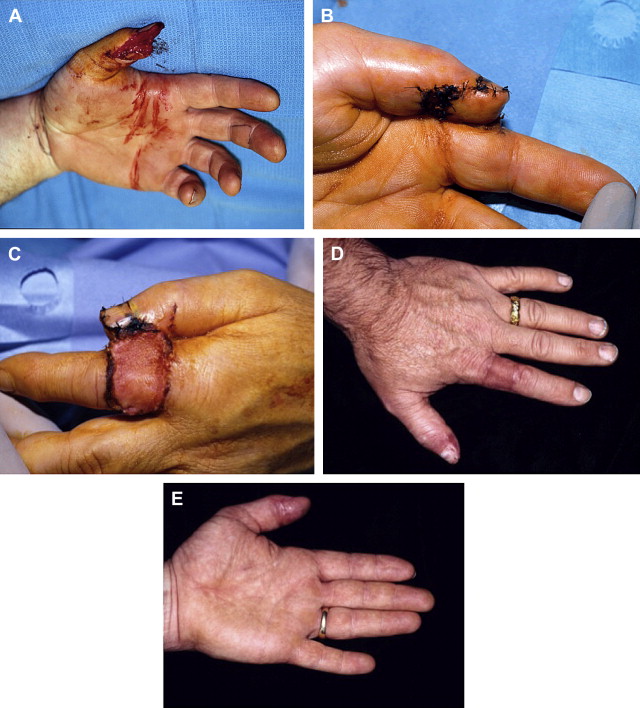
The cross-finger flap from the index finger is an excellent reconstructive technique for larger volar and tip defects of the thumb (up to 2–3 cm 2 ). The tissue transferred is reliable and durable. The chief disadvantages of this technique are thumb coaptation to the index finger for 2 to 3 weeks and the need for a skin graft on the index donor site. A radially based rectangular flap is marked on the dorsum of the index proximal phalanx ( Fig. 2 ). The flap is incised and elevated ulnarly to radially in the plane between the subcutaneous tissues and the extensor mechanism. It is very important to leave the paratenon on the extensor to allow skin grafting. When the radial aspect of the flap is reached, Cleland’s ligament must be released along the length of the base of the flap to prevent kinking at the flap hinge. The flap is then inset to the thumb. A full-thickness skin graft is sutured to the dorsum of the index finger. At 2 or 3 weeks, the flap is divided, and the inset to the thumb is completed. After division, aggressive range of motion therapy for both the thumb and index finger should begin.
The Littler neurovascular island flap is a valuable tool in thumb reconstruction. This flap is not typically used as a primary coverage flap, although it is possible to use it in that manner. The flap’s most common use is for the restoration of sensation to the thumb pulp after reconstruction. The flap is based on the ulnar neurovascular bundle of either the middle or ring finger. The ulnar side of the digit is chosen because its loss has minimal effect on grip and pinch activities. The dimensions of the flap needed are marked on the ulnar pulp of the chosen donor finger. Often, the flap requires harvesting of skin over the distal and middle phalanges of the donor finger. The flap is incised, and a midlateral or Bruner incision proceeding from the proximal aspect of the flap is made. The flap is elevated distally to proximally, and the entire ulnar neurovascular bundle is elevated in continuity with the flap. It is important to take the neurovascular bundle with a fairly thick sleeve of surrounding fatty tissue containing the vasa vasorum of the artery because that is the only source of venous outflow for the flap. Skeletonization of the artery results in venous congestion. The dissection must be done fairly proximally in the palm to allow adequate transposition to the thumb, and the other branch of the common digital artery (the radial digital artery to the ring or small finger) must be divided. The common digital nerve can undergo intrafascicular splitting to allow adequate flap mobility. The flap is transposed to the thumb via subcutaneous tunnel, or a connecting incision from the donor site to the thumb can be made. The flap is then inset into the volar defect of the thumb. The donor site is grafted with full-thickness skin. In addition to postoperative restoration of motion, patients must work with a hand therapist on sensory re-education of the thumb.
The proximally based first dorsal metacarpal artery (FDMA) flap is very useful for thumb coverage, although it is better suited for dorsal thumb defects than palmar defects. The flap’s harvest causes virtually no donor site functional loss. The FDMA is found using a Doppler device, beginning proximally with the radial artery at the anatomic snuffbox. The radial artery then branches into the princeps pollicis artery radially and the FDMA ulnarly. The flap is centered over the FDMA. It is incised and dissected distally to proximally, leaving paratenon over the extensor mechanism for later skin grafting. To ensure inclusion of the FDMA with the flap, the thin fascia over the first dorsal interosseous muscle is included with the flap. Like the neurovascular island flap, the artery should not be skeletonized because this damages the venae comitantes. Once the flap is elevated, it can then be tunneled to the thumb in the subcutaneous plane or a connecting incision can be made. The donor defect is closed with a skin graft.
Middle Third Thumb
Loss in the middle third of the thumb is more functionally limiting than that of the distal third. Therefore, the priorities are both soft tissue coverage and functional restoration. Commonly, the soft tissue coverage of amputations at this level will have been achieved acutely by revision amputation in which the skeletal components are shortened to allow primary closure.
Phalangization is a set of reconstruction techniques that increases the effective, rather than the absolute, length of the thumb. The chief component of phalangization is first webspace deepening. Webspace deepening allows better thumb excursion, specifically both palmar and radial abduction, thereby improving the thumb’s motion. First webspaces with mild or moderate tightness can be deepened with skin grafts or local tissue rearrangement (commonly Z-plasties). The main assessment of the webspace is whether the contracture is broad or a distinct linear band. If the contracture is broad, then scar contracture incision followed by skin grafting is used, whereas if the contracture is linear, local tissue rearrangement (usually Z-plasties) is the preferred treatment. Full-thickness skin grafts are usually used for the first web. A single Z-plasty can be used for a linear scar band, although 2 combined Z-plasties (4-flap Z-plasty or double-opposing Z-plasty) are uniquely suited to this anatomic area. When using either skin graft or Z-plasty for the first webspace, the adductor muscle is often tight due to scarring. A portion of the adductor muscle can be released to allow further thumb abduction before skin closure.
More significant first webspace contractures require transposition of a larger amount of vascularized tissue into the space. The dorsal hand flap can accomplish this task in a straightforward manner. This flap is proximally based on the dorsum of the hand and is vascularized by the metacarpal artery system. Unlike the FDMA flap, the dorsal hand flap is not an island flap and can include more than 1 metacarpal artery. The flap’s distal extent is at the level of the metacarpal heads and is elevated in the plane between subcutaneous tissue and extensor tendon paratenon. The flap is then transposed radially into the first webspace after release of all constraining structures in the space. The donor site is skin grafted.
If the dorsal hand skin has been injured or if a larger amount of vascularized tissue is required to resurface both the first web and the thumb itself, then regional flaps are necessary. The radial forearm flap is an excellent choice for this. The utility of the radial forearm flap has been repeatedly demonstrated in a variety of hand reconstruction settings, including the thumb. The major drawback to use of a reverse-flow radial forearm flap is that its use may compromise future thumb reconstruction. Specifically, if a microvascular toe transfer is being considered for thumb reconstruction, the radial artery is the preferred recipient vessel, and the transposition of a pedicled radial forearm flap makes the later microvascular transfer difficult, if not impossible. It is, however, possible to use a radial artery perforator flap, leaving the radial artery intact. Saint Cyr’s group has found with computed tomographic studies that a cluster of radial artery perforators exist just proximal to the wrist, making them quite suitable for thumb or first web reconstruction.
The radial forearm flap is extremity versatile and can be harvested as a fascia-alone flap, fasciocutaneous flap, or suprafascial skin flap. For thumb reconstruction, the use of the fascia-alone flap with skin grafts applied directly to the flap allows maintenance of the normal contour of the thumb, although it provides less padding than a fasciocutaneous flap. An advantage of the fasciocutaneous flap is that the lateral antebrachial cutaneous nerve can be harvested with it and coapted to the ulnar digital nerve of the thumb, thus restoring some sensation. Because of their bulk, however, fasciocutaneous flaps usually require several debulking procedures. An Allen test is always performed to ensure that the digits will remain perfused by the ulnar artery. The pivot point of the flap pedicle is approximately at the radial styloid, although it can be more proximal than this. The flap should then be marked on the forearm such that the pivot point is midway between the distal end of the thumb or first web defect and the proximal end of the radial forearm flap. The flap is elevated on the radial and ulnar sides. On reaching the ulnar edge of the brachioradialis muscle on the radial side of the flap and the radial edge of the flexor carpi radialis tendon on the ulnar side of the flap, dissection then proceeds directly down to the radius. Dissection then proceeds under the deep aspect of the radial vascular bundle. Before dividing the proximal end of the radial artery, a microvascular clamp can be placed on the artery just proximal to the flap and the tourniquet released. After several seconds, if both the flap and all the digits are well perfused, the proximal radial artery can then be divided and the flap transposed to the thumb. Depending on the type of flap used, the donor site is primarily closed (fascia-alone flap) or skin grafted (fasciocutaneous or suprafascial). Because venous outflow from the reverse radial artery flap is retrograde through the venae comitantes against the venous valves, venous congestion can occur. It is imperative to include the venae comitantes and surrounding fatty tissue with the arterial pedicle when raising the flap. Performing an antegrade venous microvascular anastomosis with the cephalic vein of the flap to a vein in the hand can reduce venous congestion and flap swelling.
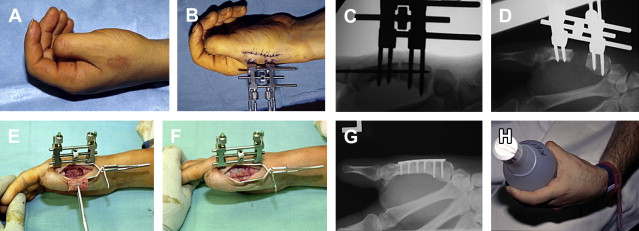
Metacarpal lengthening allows increase in the absolute length of the thumb ray ( Fig. 3 ). This procedure is usually performed for more proximal losses in the middle third of the thumb and was pioneered by Matev. Matev reported that the only absolute contraindication to the procedure is less than 3 cm of remaining thumb metacarpal. It should be explained to the patient that this reconstruction technique requires a long period with external fixation and multiple outpatient visits, and patient acceptance of the technique should be established before reconstruction. The pins for the distraction device are placed distally and proximally before osteotomy. Through a dorsal incision over the metacarpal, the distraction device is applied first, then the bone is cut at the diaphysis and the skin closed. Distraction is initiated at 1 millimeter per day until the desired length is achieved. Although in some patients, especially children, the bony gap of the metacarpal ossifies, most patients require bone grafting at a second surgery. This bone can be harvested from the iliac crest or, with small defects, from the distal radius. While the bone graft is consolidating, the original frame may be left in place or one may change the hardware to internal fixation. In Matev’s experience, several patients had first webspace creep because the distraction draws the first webskin distally. If this condition occurs, one of the first web -deepening techniques described previously may be used.
Related posts:
 Free Functional Muscle Transfer for the Upper Extremity
Free Functional Muscle Transfer for the Upper Extremity
 Scar Contractures of the Hand
Scar Contractures of the Hand
 Functional Reconstruction of the Hand: The Stiff Joint
Functional Reconstruction of the Hand: The Stiff Joint
 Current Status of Brachial Plexus Reconstruction: Restoration of Hand Function
Current Status of Brachial Plexus Reconstruction: Restoration of Hand Function
 Treatment of Nonunion and Malunion Following Hand Fractures
Intrinsic Flaps in the Hand
Treatment of Nonunion and Malunion Following Hand Fractures
Intrinsic Flaps in the Hand
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


