Injection of neurotoxin is the most commonly performed cosmetic procedure in the United States, and the total number of male patients seeking botulinum has steadily increased over the years. Because of their unique aesthetic goals, expectations, and anatomy, men require differing botulinum toxin doses and techniques. This article provides an evidence-based approach to botulinum toxin in men. Each area of the face is discussed separately, focusing on gender differences in anatomy, treatment goals, and injection method.
Key points
- •
Men have unique aesthetic goals, expectations, facial anatomy, and aging processes and thus require a tailored approach to botulinum toxin injections.
- •
Men have more skeletal muscle mass and produce greater facial movements than women and thus generally require a higher number of units of botulinum toxin.
- •
Approaches for the upper face are better supported by literature than for the lower face, but more studies are needed to further investigate gender differences.
Introduction
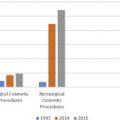
Injection of neurotoxin remains the most commonly performed cosmetic procedure in the United States, with 7.1 million cases being performed in 2016. Although men have consistently comprised 6% of the proportion of these patients, the total number has grown by 355% since the year 2000, with 428,542 injections of neurotoxin being performed in men in the year 2015. Because of this increase, providers have become more cognizant of the need to tailor their consultation and injection technique to male patients. Men have unique goals, expectations, facial anatomy, and aging processes. However, few clinical studies have evaluated gender differences in botulinum toxin dosing, technique, efficacy, and safety. This article serves as a guide for practitioners who provide injectable neurotoxins to men.
Introduction
Injection of neurotoxin remains the most commonly performed cosmetic procedure in the United States, with 7.1 million cases being performed in 2016. Although men have consistently comprised 6% of the proportion of these patients, the total number has grown by 355% since the year 2000, with 428,542 injections of neurotoxin being performed in men in the year 2015. Because of this increase, providers have become more cognizant of the need to tailor their consultation and injection technique to male patients. Men have unique goals, expectations, facial anatomy, and aging processes. However, few clinical studies have evaluated gender differences in botulinum toxin dosing, technique, efficacy, and safety. This article serves as a guide for practitioners who provide injectable neurotoxins to men.
Goals and expectations in male patients
Men generally seek cosmetic procedures in order to appear youthful. In an online survey of 600 men aged 30 to 65 years, Jagdeo and colleagues found the main reason respondents would consider a facial injectable were to look good for their age and to look more youthful. Another survey, conducted by the American Academy of Facial Plastic and Reconstructive Surgery, showed that “looking younger, work-related concerns,” and wanting to improve competitiveness were the main reasons men pursued cosmetic procedures. Because it is minimally invasive and requires no down time, botulinum toxin is an especially attractive procedure for men who wish to appear more youthful.
The pretreatment consultation is essential in preparing for a successful outcome and satisfied patient. Some men come in for a particular concern or are seeking enhancement, whereas others desire a general antiaging consultation. Therefore, it is important to ascertain the patient’s concerns and aesthetic goals. A physical examination should also be performed during the visit, assessing the patient from frontal and oblique views at rest and during facial expression, taking note of baseline asymmetries, presence of static and dynamic rhytides, and muscle mass. In addition, educate the patient on the recommended procedures, possible adverse events, and expectations. Explain that there is increased patient satisfaction with continued retreatment, and that although dynamic rhytides are most responsive, static lines can improve with repeated injection. Also, review interventions other than botulinum toxin that may be necessary to achieve optimal results, such as fillers, lasers, skin-tightening procedures, chemical or cold lipolysis, and surgery.
It is important to advise patients on common side effects, like transient edema, erythema, and bruising. Men specifically may be more likely to develop ecchymoses. Men undergoing facial plastic surgery have a higher incidence of postoperative hematoma, which may be explained by the findings that, on the face, men have higher blood vessel density, more microvessels, increased perfusion via Doppler, and larger hair follicles. In our practice, we use a 0.3-mL BD syringe with a 31-gauge, 8-mm needle (Becton Dickinson Labware, Franklin Lakes, NJ). For sensitive patients, a 32-gauge needle can provide more comfort than a 30-gauge needle.
Botulinum toxin types
Botulinum toxin is produced by Clostridium botulinum , an anaerobic, gram-positive, spore-forming rod. The bacterium produces 8 distinguishable neurotoxins. Although both types A and B are currently US Food and Drug Administration (FDA) approved, only type A toxin has indications for cosmetic use ( Table 1 ). The toxin is composed of a 100-kDa heavy chain and a 50-kDa light chain, linked by a disulfide bridge. The heavy chain binds the presynaptic neuron, allowing entry of the light chain into the cytoplasm. The light chain in turn binds and deactivates a component of the soluble N -ethylmaleimide–sensitive factor attachment protein receptor (SNARE) complex. A functioning SNARE complex is needed to release stored acetylcholine from the presynaptic neuron. Botulinum toxin types A and B have different targets within the SNARE complex.
| Generic Name | OnabotulinumtoxinA | AbobotulinumtoxinA | IncobotulinumtoxinA |
|---|---|---|---|
| Brand Name | Botox (Botox Cosmetic, Allergan, Irvine, CA) | Dysport (Galderma Pharma SA, Lausanne, Switzerland) | Xeomin (Merz Pharmaceuticals, Frankfurt, Germany) |
| Mechanism | Synaptosomal-associated protein 25 (SNAP-25) | SNAP-25 | SNAP-25 |
| Aesthetic FDA Indications (Approval Year) | Glabella (2002) Lateral canthal lines (2013) Forehead lines (2017) | Glabella (2009) | Glabella (2011) |
| Vial Sizes | 50 U 100 U | 300 U | 100 U |
| Reconstitution Volume (Concentration) | 2.5 mL for 100 U vial (4 U/0.1 mL) | 3.0 mL (10 U/0.1 mL) | 2.5 mL for 100 U vial (4 U/0.1 mL) |
| Relative Strength (OnabotulinumtoxinA/Product) | 1:1 | 1:2–1:3 (likely closer to 1:2) | 1:1 |
Aside from a unique mechanism of action, each commercially available type of neurotoxin has unique composition, complexing proteins, manufacturing, dosing, and clinical efficacy. Products are available in different vial sizes and can be reconstituted to various concentrations. Because of these dissimilarities, there is no standardized dose-response equivalence between different botulinum toxin products. The area of diffusion of botulinum toxin widens with increasing volume and concentration. Studies have shown that the field effect (action halo on muscular and sweat gland activity) is comparable among the various products if using equal volumes and equipotent doses. The approximate dose conversions in Table 1 have been obtained from experimental studies and consensus guidelines. For the remainder of this article, recommended doses are based on onabotulinumtoxinA (OBA), unless otherwise specified.
Although the body of literature comparing different botulinum toxin types is growing, the study of gender differences in response to botulinum remains sparse. Only 3 studies have examined male-specific dosing, all to the glabella. Although the specifics of each study are discussed later, they support the use of greater botulinum toxin doses in men, which is likely because men have a greater muscle mass. Studies have shown that men have a greater skeletal muscle mass, influenced by the anabolic effect of androgens. In addition, men produce greater facial muscle movements. The findings that men have greater muscle mass and facial movements supports the suggestion that men need higher doses of botulinum toxin than women to achieve comparable results. Nevertheless, not all male patients and treatment areas require higher doses. In some instances, the goal may be to reduce rather than eliminate muscle activity. This article discusses the aesthetic use of botulinum toxin in male patients by location on the face and neck, pointing out gender-specific differences in anatomy, goals, dosing, and injection technique.
Upper face
Forehead
Neurotoxin can be used in the frontalis muscle to decrease the presence of transverse forehead lines. In their online survey, Jagdeo and colleagues found that the forehead is the third most likely area to receive treatment in male patients.
Anatomy
The frontalis muscle is the only brow elevator. The muscle originates from the galea aponeurotica in the scalp, and inserts into the subcutaneous tissue and deep dermis above the superciliary arch. Some fibers interdigitate with the corrugator supercilii, procerus, and orbicularis oculi muscles. Compared with women, the forehead in men has a greater height and width. In addition, the presence of androgenetic alopecia further increases the height of the forehead. There are also differences in brow shape and location: the male brow is straighter, more horizontal, and sits lower on the orbital rim. A Japanese study examining the facial wrinkles of 173 men and women aged 21 to 75 years showed that men had more severe forehead lines than women at all ages.
Treatment goals
Although neurotoxin can completely immobilize the forehead, goals must be discussed with the patient. The presence of rhytides can impart a more distinguished appearance to the male face. Therefore, softening the horizontal lines while still allowing some movement is often preferred in men. In addition, the position and shape of the brow is of utmost importance when discussing aesthetic goals. An arched brow can feminize the male face, whereas a brow that sits too low can interfere with vision, cause a heavy sensation, and impart an aged and antagonistic appearance.
Dosing and injection technique
- •
The consensus recommendations for the forehead are a total of 8 to 25 units, placing 2 to 4 units in 4 to 8 injection points ( Fig. 1 ).
Fig. 1
A 52-year-old man before ( A ) and after ( B ) 36 units of abobotulinumtoxinA to the forehead (injection points are indicated by blue dots ). Note the extra injection point in the frontotemporal hair line where the hairline recedes.
- •
Injections are best placed intramuscularly in horizontal rows, with purposeful injection of the lateral frontalis in order to prevent arching of the brow. However, in men with lower-set eyebrows, keep the injection points higher on the frontalis to prevent excessive heaviness of the brow. Some experts use a lower dose per unit volume for injections into the dermis in the lower frontalis, because they believe this technique can improve rhytides in the lower forehead without causing brow descent.
- •
Staying at least 1 cm above the orbital rim avoids diffusion of neurotoxin into the levator palpebrae superioris, which can result in upper eyelid ptosis.
- •
In men with androgenetic alopecia, also place injection points on the frontal scalp to prevent an unnatural wrinkling in this area ( Fig. 2 ).
Fig. 2
In men with androgenetic alopecia, injection points should be extended into the frontal scalp.
Glabella
Men tend to have a deeper furrow in the glabella because of their anatomy. Botulinum toxin injection can soften the glabellar ridge and decrease the appearance of aggressiveness and age. The glabella was the fourth most common area of concern in the survey by Jagdeo and colleagues.
Anatomy
Two corrugator supercilii, depressor supercilii, and a procerus contribute to glabellar lines. The corrugators originate from bone in the medial brow ridge and run along the orbital rim, ending more laterally and superiorly onto the frontalis muscle. The corrugator supercilii extends farther laterally in men. Vertical glabellar lines are formed by the corrugators. Anatomic studies have shown that the depressor supercilii originates from the frontal process of the maxilla, about 1 cm above the medial canthal tendon, traveling superiorly 4 to 5 mm before inserting into the dermis in the medial brow. It acts as a brow depressor and may contribute to oblique glabellar lines. The procerus fibers originate from tendons in the inferior nasal bone, and interdigitate superiorly with the frontalis. Contraction of the procerus causes horizontal glabellar lines. In men, the glabella is wider and projects more anteriorly. A study showed that men less than 65 years of age had more severe glabellar lines than women of the same age, although this was only statistically significant between ages of 21 and 28 years.
Treatment goals
Unlike other areas of the face, total effacement of glabellar lines is often desired in male patients. Immobilizing the glabella alone can result in lifting of the lateral brow, because of unopposed action of the frontalis. Thus, when treating the glabella in male patients, it is prudent to also treat the forehead.
Dosing and injection technique
- •
The glabella is the only location where the dose of botulinum toxin was specifically studied in men. Carruthers and colleagues injected the glabella of 80 male patients with 20, 40, 60, and 80 units of OBA. They found doses of 40 to 80 units were most effective and had the greatest duration compared with 20 units, without an increase in adverse events. A previous study by the same investigators had shown that, in female patients, the glabellar complex should be treated with at least 20 units. Carruthers and colleagues recommend starting with 40 units in the male glabella.
- •
Brandt and colleagues showed that, in 15 male and 90 female patients injected with 50 units of abobotulinumtoxinA (ABO), 67% of men, compared with 93% of women, obtained significant improvement of glabellar lines. The investigators concluded that men may need ABO doses greater than 50 units. Another trial supported the use of higher doses of ABO in men (60–80 units).
- •
Two injections points are indicated for each corrugator, and 1 for the procerus ( Fig. 3 ).
Fig. 3
A 49-year-old man before ( A ) and after ( B ) 30 units of onabotulinumtoxinA and 0.4 cm 3 of hyaluronic acid filler to the glabella. It is important to maintain some level of movement in the glabellar complex in a man, for a more natural aesthetic.
- •
When injecting the corrugators, stay at least 1 cm above the orbital rim to prevent diffusion into the levator palpebrae superioris. For the medial injection, identify the point of greatest muscle contraction. For the tail of the corrugator, Bloom and colleagues recommend identifying the most lateral aspect of the corrugator (presence of dimpling) and placing the lateral injections just medial to this insertion point in the skin.
- •
Injections placed too superiorly in the mid glabella may also affect the medial frontalis, resulting in elevation of the lateral brow.
- •
Avoid injecting the glabella alone in order to prevent elevation of the brow.
Periocular Skin
Like women, men develop periocular rhytides with age. Jagdeo and colleagues’ survey found that, along with the tear trough, the crow’s feet is the facial area mostly likely to be treated in men.
Anatomy
The orbicularis oculi is a spherical muscle consisting of a lacrimal, palpebral, and orbital portion. The orbital portion controls voluntary closure of the eyelids, creating dynamic lateral canthal lines. With time, these lines become static. In men, the orbicularis oculi is broader and extends more laterally. Men also tend to have predominantly a lower-fan pattern of lateral canthal lines, with greater recruitment of muscular elevators of the cheek. In addition, the orbicularis oculi contributes to the palpebral aperture and infraorbital shelving and rhytides.
Treatment goals
Lateral canthal lines in men can indicate maturity and contribute to attractiveness and the appearance of a positive disposition. Thus, a goal for male patients may be just to soften these rhytides.
Dosing and technique
- •
The FDA approved the use of OBA for lateral canthal lines in 2013. A phase 2 dose-ranging study showed that there was a greater responder rate with a total dose of 24 units rather than 6 or 12 units. Of the 162 patients, only 11.1% were men, and no subgroup analysis was performed. The consensus recommendation for lateral canthal lines is 6 to 15 units per side. For men, Flynn recommends starting with 15 units of OBA per side.
- •
The most used technique for lateral canthal lines involves 3 injections ( Figs. 4 and 5 ). One injection is placed at the level of the lateral canthus, 1 cm lateral to the orbital rim. The other 2 are placed 1.0 to 1.5 cm both superiorly and inferiorly, angled at 30° anterior to the first injection. In patients with a lower-fan pattern of canthal lines, the other 2 injections can be placed anterior and inferior to the first injection. Some investigators add microdroplets (0.5 units) of toxin to the lateral inferior orbicularis oculi for lower fanning lines. It is important to inject superficially, because the zygomaticus major may be as shallow as 0.41 cm deep to the orbicularis oculi. Diffusion into the zygomaticus major or levator labii superioris can affect the smile. In addition, because men can have greater lateral fanning of the orbicularis oculi, a second row of injections is sometimes used.
Fig. 4
A 42-year-old man before ( A ) and after ( B ) 12 units of onabotulinumtoxin A to each orbicularis oculi.
Fig. 5
Injection points for targeting the orbicularis oculi in a man with full-fan pattern of periocular rhytides, with a total of 12 units of onabotulinumtoxin A or 36 units of abobotulinumtoxinA per side.
- •
Applying 1 to 2 units per side of OBA to the infraorbital eyelid (inferior orbicularis oculi muscle) can decrease lower eyelid rhytides and shelving, and increase the palpebral aperture. In a study of 15 women, this injection was shown to increase the palpebral aperture at rest by a mean of 0.5 mm, and by 1.8 mm if combined with treatment of lateral canthal lines. The toxin is applied in the midpupillary line, 3 to 4 mm inferior to the lid margin. Before this injection, the physician should assess for lower scleral show and perform a snap test. Men have been found to have a greater degree of lower eyelid sagging, which increases the risk of adverse events with an inferior eyelid injection. In addition, the presence of lower eyelid and malar mound edema should be noted. Neurotoxin injection to the lower eyelid caused lower eyelid edema in 1% of patients in phase 3 trials.
Midface
Nose
In 2015, rhinoplasty was the most common procedure performed in men. Because of the growing popularity of nonsurgical rhinoplasty, more men may seek hyaluronic acid filler and botulinum toxin to improve the appearance of their nose.
Anatomy
Various muscles contribute to the position and rhytides of the nose. The nasalis has a transverse and alar portion. The alar nasalis, present over the nasal ala, is involved in nasal flaring. Contraction of the transverse nasalis produces nasal oblique lines (also known as bunny lines). The depressor septi nasi causes the downward movement of the nasal tip during activities like speaking and smiling. This muscle arises from the orbicularis oris and periosteum above the central and lateral incisors, then inserts onto the nasal septum or medial cura. It is notable that the levator labii superioris alaeque nasi (LLSAN), procerus, orbicularis oculi, and zygomaticus major and minor also play a role in nasal movements and wrinkling.
Treatment goals
Patients who have had botulinum toxin to the upper face may notice that oblique nasal lines become more evident. The presence of oblique nasal lines has not been studied in men, but physicians should still assess for this possible area of concern ( Fig. 6 ). Another concern for which men may seek treatment is nasal tip ptosis. As men age, the nasal tip descends. In patients in whom the ptosis worsens with muscle activity, botulinum to the depressor septi nasi may help. Excessive nasal tip elevation may feminize the patient, because the angle between the upper cutaneous lip and nasal tip tends to be 97° in men versus 104.9° in women.