The superficial circumflex iliac artery perforator flap is evolved from the groin flap, which was one of the early free flaps with a good concealed donor site. By further understanding the anatomy of perforators and elevating the flap based on it, this will provide added advantage of being a thin flap, harvesting as a composite flap, and help estimate the limit of skin paddle dimension. Despite these advantages, the relatively short pedicle still remains a challenge where long pedicle flaps are needed. One should select the flaps based on the recipient defect condition along with surgeons’ experience, knowledge, and preference.
Key points
- •
The superficial circumflex iliac artery perforator flap is one of the thinnest flaps available based on the perforator from the superficial circumflex iliac artery.
- •
One must understand the anatomy of the perforators, as the flap can be elevated on either the medial (superficial) or lateral (deep) branch or both.
- •
The design of the flap will vary depending on the branch used: medial branch will provide a medium or large-sized flap based on the perforator pattern (anchoring vs axial), whereas lateral branch will have an axial pattern allowing to harvest a flap extending into the flank.
- •
The flap can be harvested as a chimeric flap with lymph nodes, bones, and part of a muscle.
- •
It has a very well-hidden donor scar.
Introduction
Free flap approach is inevitable when defects are complex exposing essential structures such as tendons, bones, nerves, and joints. In the lower extremity this region remains to be the lower leg, ankle, and foot. Even for a moderate-size defect, local solutions will not be enough and free flaps will be required to cover the defect. Once free flap is planned, multiple other challenges arise. In the age where aesthetic outcome is as important as function, one must consider a thin flap for the anterior surface of the tibia, as this region is naturally thin and consider a flap with a skin paddle resembling the natural skin surface. Donor site morbidity such as potential loss of muscle function or a large scar can also be an issue. It is within this regard that the superficial circumflex iliac artery perforator (SCIP) flap deserves attention to reconstruct defects for lower extremity.
The SCIP flap is an evolution from groin flap. The groin flap, supplied by the superficial circumflex iliac artery (SCIA), is one of the first free flaps successful in reconstruction. This flap was first described as a pedicle flap by McGregor and Jackson and then introduced as a free flap by Daniel and Taylor. , This flap was the workhorse flap during the early period of microsurgery as required for lower extremity reconstruction provides a hidden scar and a large cutaneous tissue. However, its use for lower extremity slowly faded away, as introduction of muscle flaps was perceived to function better in extremities against infection and because the short pedicle of the groin flap made it difficult to use when longer pedicle was needed. Other disadvantages of groin flap were variable arterial anatomy, donor/recipient vessel size disparity, bulky flap in obese patients, and donor site seroma collection. ,
It was not till Koshima and colleagues revisited the groin flap and modified it as a skin flap elevated above the deep fascia based on the SCIP that the groin region as a free flap regained recognition. The SCIP flap was able to overcome some disadvantages such as bulkiness and variable arterial anatomy by using the free-style free flap approach. , But even with these evolved technique and concept, the SCIP flap was still challenging to use due to the short pedicle, small vessel caliber, relative bulkiness especially in obese patients, and donor site morbidity such as lymphorrhea. Further modifications were made where Hong and colleagues harvested the flap on the superficial fascia making the flap thinner (super-thin flaps) while avoiding injuries to the lymphatic system, which is located on the deep fat below the superficial fascia, thus minimizing lymphorrhea. , Further studies clarified the superficial (medial) branch and deep (lateral) branches of SCIA as well as the venous outflow, which helped to achieve better design, vascular supply, harvest multiple composition, and understand the limit of the flap. , , Although both medial and lateral branch stems from the SCIA, it can be seen as 2 different flaps based on each perforating branch, as it provides very distinctive and unique characters. In this article, the author reviews the surgical elevation technique, benefits, and indications of the SCIP flap for lower extremity reconstruction.
Indications and contraindications
The indications for the SCIP flap will be for defects that need to use the merits of the flap. The most commonly applied indication will be for lower extremity defects that require a thin flap coverage especially in the anterior surface of the leg and the ankle region. The SCIP flap has replaced the anterolateral thigh (ALT) flap as our workhorse flap for simple resurfacing of the leg. When a large flap has to be harvested, using the lateral branch allows to harvest the skin extending to the abdominal flank region. If lymph node is required to treat lymphedema or prevent potential development of lymphedema on the contralateral limb, harvesting 1 or 2 lymph nodes with the skin paddle may be indicated. Soft tissue defects with small bone gaps of the leg or foot that needs simultaneous bone and skin coverage is another good indication. The use of skin flaps for chronic osteomyelitis has been shown to have no difference in outcome and the same can be said for the SCIP flap. When a small dead space is noted, part of the flap can be deepithelialized to obliterate the dead space.
The main contraindications for the SCIP flap would be defects that need a long pedicle to reach the recipient vessels. Although one can safely perform vessel grafts to extend the pedicle length, the chances for complication may increase and require more surgical time. Another contraindication would be when the groin region has prior surgery potentially altering the anatomic structure of the SCIA. The vascular structure can be confirmed by using the Duplex ultrasound, but the multiple scars in this region can have a negative effect on the circulation of the flap. A relative contraindication would be defects that exceed the coverage potential of the SCIP flap and unable to close primarily. Although one can perform skin grafts for the donor defect, it would be less ideal to use the advantages of the flap. The authors also recommend to avoid harvesting the SCIP flap on the side that underwent percutaneous angiograms or angioplasty before surgery. When hematoma is collected, it makes identifying the perforators very difficult.
Preoperative evaluation and special considerations
Using an SCIP flap helps to (1) obtain a thin flap, (2) have reliable perforator anatomy (medial and lateral branches) and superficial vein, (3) have the capability to either elevate a small or a large flap (from 4 × 3 cm to 12 × 35 cm), (4) have a primarily closed hidden donor scar, and (5) elevate as a composite flap (including lymph nodes, iliac bone, and part of Sartorius muscle). The disadvantages of using SCIP flap include (1) a relatively short pedicle and (2) small perforator artery diameter ( Table 1 ).
| Pros | Cons |
|---|---|
| Well-concealed donor site | Smaller vessel lumen |
| Thin and pliable skin flap—allows single-stage resurfacing | Short pedicle |
| Septocutaneous pedicle (medial branch) | Learning curve to elevate as thin flap |
| Expedient harvest | Supermicrosurgery technique required for certain defects |
| Composite with lymph node and bone | |
| Medium to large skin dimension |
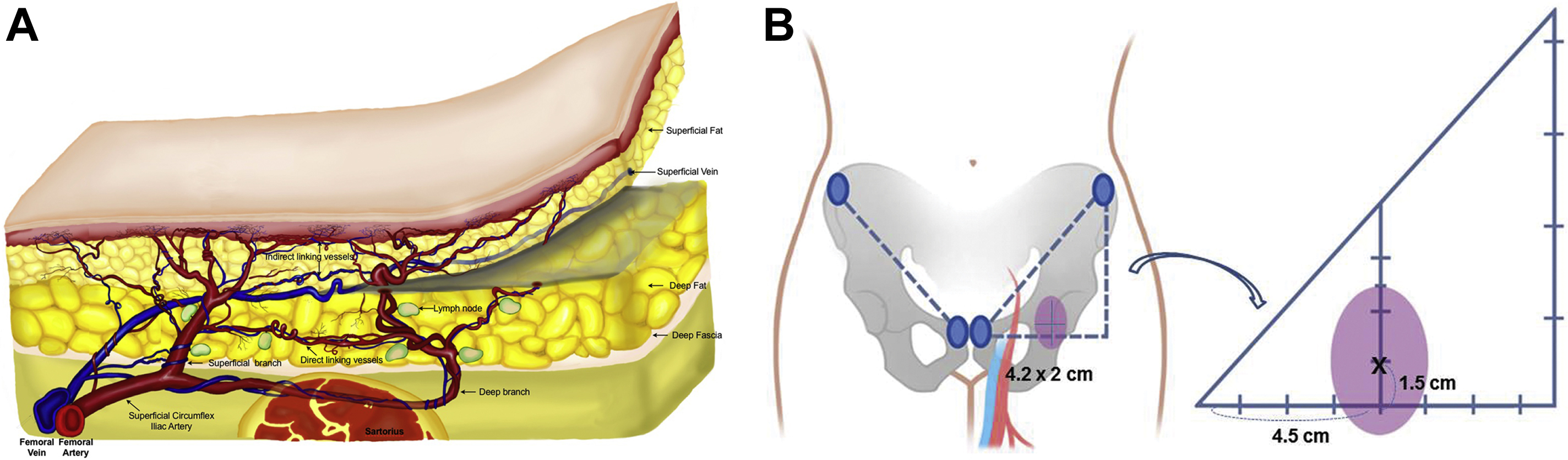
Preoperative ultrasound Doppler is used to mark the potential perforators of the SCIP flap. In 95% of the SCIP flaps, the medial perforators of the SCIA penetrate the deep fascia within an oval of 4.2 × 2 cm (vertical x horizontal) with the center of the oval point located 4.5 cm lateral and 1.5 cm superior from the superolateral corner of the pelvic tubercle. The medial perforating branch then can be divided into 2 distinctive patterns. The axial pattern (44%) shows the perforator runs in an axial pattern on the superficial fat passing the anterior superior iliac spine (ASIS) reaching the flank region, whereas the anchoring pattern (56%) displays the perforator reaching the subdermal plexus without further branching. This anatomy becomes relevant especially when longer SCIP flaps need to be harvested, for which the axial pattern would be safer to use. The deep branch can be detected on the lateral region of the axis drawn from the pubic tubercle to the ASIS. It usually travels laterally beneath the deep fascia and often with an intramuscular pathway perforating the deep fascia on the lateral aspect (deep branch) near the ASIS. The computed tomography angiogram allows to visualize the medial (deep) and lateral (superficial) branches with accuracy, allowing safer design especially in respect to size of the flap. Recently, the use of ultrasound has helped to define not only the exact location but also the pathway of the perforator and the superficial vein as well with high accuracy. One should remember that the SCIP flap can be designed based on either the medial and lateral perforators or both when needed ( Fig. 1 ). Table 2 shows the points to consider when selecting either the medial or lateral branch of the SCIA of the SCIP flap.
| Medial (Superficial) Branch | Lateral (Deep) Branch |
|---|---|
| Septocutaneous perforator | Muscular path included |
| Short pedicle | Relatively longer pedicle |
| Topographically constant perforator | Nonconstant perforator |
| Mostly axial pattern perforator |
| Medium size skin paddle (anchoring type) Large size skin paddle (axial pattern) | Large size skin paddle |
| Expedient harvest | Slower harvest |
| Composite with lymph node | Composite with bone and muscle |
Related posts:
 Propeller Flaps in Lower Extremity Reconstruction
Propeller Flaps in Lower Extremity Reconstruction
 Free-Style Free Perforator Flaps in Lower Extremity Reconstruction
Free-Style Free Perforator Flaps in Lower Extremity Reconstruction
 Free Flaps in Lower Extremity Reconstruction
Free Flaps in Lower Extremity Reconstruction
 Orthoplastic Approach to Lower Extremity Reconstruction
Orthoplastic Approach to Lower Extremity Reconstruction
 The Anterolateral Thigh Perforator Flap
The Anterolateral Thigh Perforator Flap
 Lower Extremity Reconstruction in the Pediatric Population
Lower Extremity Reconstruction in the Pediatric Population
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


