Skindex-29 and Skindex-16 are validated measures of the effects of skin diseases on patients’ quality of life. This article reviews the development of both versions of Skindex, discusses their measurement properties and interpretability, and gives examples of how they have been used and adapted for dermatologic research internationally. Studies of quality of life in patients with nonmelanoma skin cancer are described to illustrate the use of Skindex to understand quality of life and to compare effectiveness of different treatments for this highly prevalent condition.
In practicing dermatology one soon realizes that the severity of most skin diseases is not easily assessed and communicated. Most skin conditions cannot be followed by laboratory values, and typically patients survive with (rather than die from) their diseases. Also, one quickly learns that the visible extent of disease often does not correlate with the degree to which patients are disturbed by it; patients with minimal clinical involvement may be highly distressed, but others with extensive involvement may not be bothered. The severity of a skin disease is related both to its clinical extent (using clinimetric measures) and its effects on patients’ quality of life (using psychometric measures).
This article describes how the author and her colleagues designed and worked with a measure of the effects of skin disease on quality of life, called Skindex. The article reviews the development of the two versions of Skindex, discusses their measurement properties and interpretability, and gives examples of how they have been used and adapted for dermatologic research internationally. Specifically discussed are studies of quality of life in patients with nonmelanoma skin cancer (NMSC), to illustrate how Skindex has been used to understand quality of life and to compare effectiveness of different treatments for this highly prevalent condition.
Development of Skindex
When we began to develop Skindex, we were greatly informed by the previous work of Finlay and coworkers on measuring disability from skin disease. Our goal was to develop an instrument to measure comprehensively the effects of skin disease on health-related quality of life, and we specifically designed the instrument to be able to discriminate between patients with different effects and to detect changes in patients over time. An incremental strategy was followed that began with a hypothesis: based on a literature review of previous clinical and psychologic studies and substantial input from patients and clinicians, we constructed a comprehensive conceptual framework for the ways in which we hypothesized skin diseases affected patients. Survey items were composed to measure all domains in the framework, and then the hypothesis was tested by examining the validity of the items in a series of psychometric tests using the responses of a large sample of patients.
Original Conceptual Framework
We proposed that skin diseases affect patients in either psychosocial or physical ways. We suggested that psychosocial effects could be cognitive (beliefs about self or others); social; or emotional. Subdimensions of emotional effects include depression, fear, embarrassment, and anger. Physical effects are either discomfort or limitations in physical functioning. This original hypothesized framework is depicted in Fig. 1 .

Item Composition and Prototype Skindex
The team consisted of two psychometricians, and using conventional principles we composed 65 items to assess the dimensions in the conceptual framework. This draft survey was pilot-tested and ambiguous and redundant items were changed or deleted, which left a 61-item prototype version of Skindex. The measurement properties of this trial version were tested in a series of studies that demonstrated it to be reliable and to have substantial evidence of validity as a measure of the effects of skin disease on quality of life.
Refinement into Skindex-29
We wanted to improve the ability of the prototype Skindex to discriminate among patients with likely different degrees of quality-of-life effect, and to be more sensitive to even modest changes in patients’ experiences over time. We also wanted to shorten the instrument to make it more useful in research and clinical settings. To accomplish these goals, the performance of each item was assessed, using not only qualitative judgments but also based on a priori criteria for suboptimal item performance, including reproducibility, discriminant validity, complexity, ambiguity, response distribution, and item-total correlation. The factors, or themes, that explained the variability in responses to the psychometrically soundest items were analyzed, which permitted us to test and refine the theorized model for the effects of skin disease on quality of life. Finally, we composed new items that we judged would improve discriminative and evaluative capability of the instrument.
This sequential process generated a refined conceptual framework. We now propose that the effects of skin disease on quality of life can be understood in three domains: (1) symptoms, (2) emotions, and (3) functioning ( Fig. 2 ). The analyses yielded a 29-item version of Skindex that remained reliable and valid, but that had reduced respondent burden, and improved discriminative and evaluative capability.
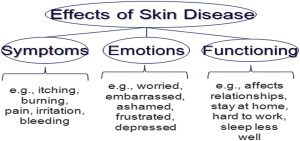
Skindex-29 inquires about how often (never, rarely, sometimes, often, all the time ) during the previous 4 weeks the patient experienced the effect described in each item. Seven items address the symptoms domain, 10 items the emotional domain, and 12 items the functioning domain. All responses are transformed to a linear scale of 100, varying from 0 (no effect) to 100 (effect experienced all the time). Skindex scores are reported as three scale scores, corresponding to the three domains; a scale score is the average of a patient’s responses to items in a given domain.
Construction of Skindex-16
Longitudinal research studies often require waves of data collection with lengthy survey instruments to assess multiple aspects of patients’ experience. We sought to develop a version of Skindex that would remain accurate and responsive as a measure of skin-related quality of life, but that would be brief (contained on one page). Also, we wanted to assess not only how often patients have a particular experience, but how much they are bothered by it. Thus, Skindex-29 was used as the substrate for a series of studies that developed a different, single-page version, Skindex-16. We used item analyses similar to those described previously to select only those items that performed well according to the criteria, and eliminated items to which most patients responded “never.” New items were composed to address aspects of quality of life that patients mentioned often in their qualitative responses but that had not been addressed in Skindex-29. This process generated a new instrument, which fits on a single page. The header inquires “During the past x weeks, how often have you been bothered by…” The response choices are on a continuous bipolar scale with seven boxes anchored by the words “never bothered” and “always bothered” at each end. As with the parent instrument, scores vary from 0 (no effect) to 100 (effect experienced all the time), and responses are aggregated in symptoms (four items), emotions (seven items), and functioning scales (five items). The performance of this new instrument, Skindex-16, was tested in more than 500 patients, and it was reliable, retained substantial evidence of validity, and was responsive to clinical change.
Choosing between Skindex-29 and Skindex-16
The Skindex instruments are copyrighted to ensure standardization in their use and scoring; permission to use either version is obtained through the non-profit MAPI research trust ( http://www.mapi-trust.org/ ). Investigators often inquire about which of the two versions they should use for their studies. This decision typically depends on the research question being addressed. Because it is longer, Skindex-29 is more comprehensive, and it might be more suitable if the goal of a project is to investigate and understand the effects of a given condition on quality of life. Also, because Skindex-29 is older and has been used more broadly in clinical research, typical scores of patients with different skin conditions are widely available and can be compared with those of patients with the disease in question. For example, we were interested in learning more about quality-of-life effects from vulvodynia, a highly painful vulvar condition that is poorly understood. We used Skindex-29 in a large sample of women and determined that those with vulvodynia were substantially more likely than those with other vulvar conditions to have feelings of depression, anger, and frustration, and to report that the vulvodynia affected broad aspects of their social and physical functioning.
Skindex-16, however, consists of the items that had the best performance characteristics in the longer instrument, and additional items that are not in Skindex-29, but that address aspects of skin disease that many patients had mentioned in response to qualitative research (eg, bother from the persistence or reoccurrence of the skin condition). Also, Skindex-16 measures bother rather than frequency of experience, which we reasoned may more directly assess effects on patients’ quality of life. Finally, because it has been refined into a single page, Skindex-16 is useful for studies in which respondent burden is a concern. For example, we have used Skindex-16 in waves of data collection over 10 years in a longitudinal study of more than 1500 patients with NMSC, as part of research to document and compare outcomes after therapy, as described later.
Choosing between Skindex-29 and Skindex-16
The Skindex instruments are copyrighted to ensure standardization in their use and scoring; permission to use either version is obtained through the non-profit MAPI research trust ( http://www.mapi-trust.org/ ). Investigators often inquire about which of the two versions they should use for their studies. This decision typically depends on the research question being addressed. Because it is longer, Skindex-29 is more comprehensive, and it might be more suitable if the goal of a project is to investigate and understand the effects of a given condition on quality of life. Also, because Skindex-29 is older and has been used more broadly in clinical research, typical scores of patients with different skin conditions are widely available and can be compared with those of patients with the disease in question. For example, we were interested in learning more about quality-of-life effects from vulvodynia, a highly painful vulvar condition that is poorly understood. We used Skindex-29 in a large sample of women and determined that those with vulvodynia were substantially more likely than those with other vulvar conditions to have feelings of depression, anger, and frustration, and to report that the vulvodynia affected broad aspects of their social and physical functioning.
Skindex-16, however, consists of the items that had the best performance characteristics in the longer instrument, and additional items that are not in Skindex-29, but that address aspects of skin disease that many patients had mentioned in response to qualitative research (eg, bother from the persistence or reoccurrence of the skin condition). Also, Skindex-16 measures bother rather than frequency of experience, which we reasoned may more directly assess effects on patients’ quality of life. Finally, because it has been refined into a single page, Skindex-16 is useful for studies in which respondent burden is a concern. For example, we have used Skindex-16 in waves of data collection over 10 years in a longitudinal study of more than 1500 patients with NMSC, as part of research to document and compare outcomes after therapy, as described later.
Interpretation of scores
To use quality-of-life measures to study disease and improve patient care, one needs to know not only raw scores, but also what the scores mean with respect to severity of effect and comparison with other patients. Because the Skindex instruments are generic in the sense that they can be used in patients with skin disease of any sort, valuable information can be obtained by comparisons of mean scores of groups of patients with certain diseases. Table 1 contains mean Skindex scores in unselected groups of patients with a variety of skin conditions.
Related posts:
 Health-Related Quality of Life in Dermatology: Introduction and Overview
Overview of Health Status Quality-of-Life Measures
Melasma Quality of Life Measures
Quality-of-Life Instruments: Evaluation of the Impact of Psoriasis on Patients
Clinical Meaning in Skin-specific Quality of Life Instruments: A Comparison of the Dermatology Life Quality Index and Skindex Banding Systems
Future Directions in Dermatology Quality of Life Measures
Health-Related Quality of Life in Dermatology: Introduction and Overview
Overview of Health Status Quality-of-Life Measures
Melasma Quality of Life Measures
Quality-of-Life Instruments: Evaluation of the Impact of Psoriasis on Patients
Clinical Meaning in Skin-specific Quality of Life Instruments: A Comparison of the Dermatology Life Quality Index and Skindex Banding Systems
Future Directions in Dermatology Quality of Life Measures
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


