Fig. 16.1
PIH 2 months following QS Nd:YAG 1064-nm laser using convention treatment protocol for treating melasma. This patient was treated with QS Nd:YAG 1064 nm 4 ns pulsed duration and fluence of 8 J/cm2 (Photograph courtesy of National Skin Centre, Singapore)
16.2 Laser and Light Therapies
16.2.1 The Q-Switched Lasers (Pigment Lasers)
The Q-switched (QS) lasers are lasers with short pulse duration in nanosecond domain. They are suited to treat pigmentary skin disorders because of melanin’s short thermal relaxation time and absorption spectrum. These lasers include the QS ruby, alexandrite, and Nd:YAG lasers. The QS lasers are wonderful devices for removing tattoos, nevus of Ota, Hori’s nevus, lentigines, and some other pigmentary disorders. Initially, it was thought that adopting the same treatment protocol used to treat other pigmentary skin disorders will also be suitable for melasma [2, 3]. But experience showed that they are not, as severe PIH is common and often no improvement could be achieved.
Taylor reported eight patients with melasma or PIH treated with the QS ruby laser (694 nm, 40 ns pulse duration) at fluences of 15–7.5 J/cm2. It was shown that regardless of fluence, there was no permanent improvement of their melasma; in some cases, darkening of melasma was even observed. Histologic sections of biopsy specimens taken before and after treatment showed extracellular melanin immediately after the procedure. Several months after the last treatment, epidermal pigmentation was back to baseline levels, and dermal melanophages were focally increased [4].
Given these results, the Q-switched lasers used in conventional treatment parameter for pigmentary skin lesions are not a recommended method to treat melasma.
16.2.2 Ablative Skin Resurfacing (Erbium: Yttrium-Aluminum-Garnet Lasers)
The erbium:YAG laser (Continuum Biomedical, Dublin, CA) emits 2940-nm laser wavelengths. This wavelength is highly absorbed by tissue water as its chromophore and is an effective ablative resurfacing wavelength. Manaloto et al. treated ten patients of Fitzpatrick skin phototypes II–V with refractory melasma using the erbium:YAG laser. Utilizing MASI scores and spectrophotometer for assessment, the authors found that there was improvement immediately after the laser treatment. However, all patients developed PIH after 3–6 weeks follow-up, despite prophylaxis oral steroids for 5 days post procedure [5].
While the PIH improved with serial glycolic acid peels, this side effect appears to outweigh the benefit derived from this ablative procedure.
16.2.3 Combination of Carbon Dioxide and QS Alexandrite Laser
Various combination treatments with ablative laser resurfacing with the QS lasers were tried too, but the problem of post-inflammatory hyperpigmentation remained.
Theoretically, pulsed CO2 laser wavelength targets water as its chromophore and can be helpful in removing epidermal pigmentation. The QS alexandrite laser emits 755 nm wavelength energy that targets melanin up to the dermis. A study reported the combination of the CO2 laser ablation followed by the QS alexandrite laser treatment to enhance the penetration of the pigment laser to remove dermal melanin in melasma. Nouri et al. treated eight patients with Fitzpatrick skin phototypes IV–VI with dermal melasma who were pretreated with 14 days of 0.05 % tretinoin cream, 4 % hydroquinone cream, and 1 % hydrocortisone cream twice daily. Four patients were randomized to receive spot treatment with one pass of the CO2 laser, followed by one pass of the Q-switched alexandrite laser. The other four patients received treatment with one pass of the CO2 laser alone. Using blinded subjective investigator evaluation as the primary end point, the authors felt that the combination therapy led to better resolution of the treated area with less peripheral hyperpigmentation. However, the sample size was small, as was the area being treated, limiting the generalizability of these results [6].
Niwat et al. reported a split-face study among Thai patients with refractory melasma on the efficacy of the Q-switched alexandrite 755-nm laser (Accolade; Cynosure, Chelmsford, United Kingdom) with or without one pass of the Ultrapulse CO2 laser (Coherent, Palo Alto, CA). Among the six females with Fitzpatrick skin phototypes II–V with refractory melasma who were treated, there was no statistically significant difference between the two treatment modalities at the end of the study. MASI and melanin index evaluation, however, showed Ultrapulse CO2 laser + QSAL gave better improvement but more severe PIH. Importantly, three (33 %) patients with Fitzpatrick skin phototypes IV–V had PIH on both sides at 2–4 weeks lasting up to 3 months, and one patient had transient hypopigmentation lasting 6 months. The authors’ conclusion was that given the risk of postoperative dyspigmentation, neither modality was safe for routine use for treating melasma in Asians [7].
It is generally felt that combination ablative and pigment lasers are not a recommended treatment for melasma in view of the high risk of PIH among Asians.
16.2.4 Fractional Laser Resurfacing
Fractional laser resurfacing is a procedure that uses laser light to create scattered microzones of thermal damage on the skin. It does not cause confluent full-thickness skin wounds, and the in-between normal undamaged skin acts as a reservoir to regenerate the laser damaged skin. This results in more rapid skin repair and recovery [8]. This laser is approved by the Food and Drug Administration (FDA) for the treatment of melasma, periorbital rhytides, pigmented lesions, skin resurfacing, acne scars, and surgical scars [9]. The microthermal zones of injury limit the area of the skin that is damaged with each treatment, which may decrease the risk of PIH.
The transepidermal elimination of debris and tissue through the microthermal treatment zones after injury could serve as an effective method of removing dermal melanophages [10]. Good clinical results may be seen in some patients (Fig. 16.2).
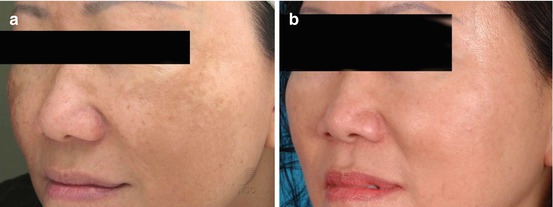
Fig. 16.2
Significant improvement of melasma after three treatments at monthly interval with non-ablative fractional laser. But recurrence appeared 3 months after stopping treatment (Photographs courtesy of National Skin Centre, Singapore)
Roshkar evaluated ten patients with Fitzpatrick skin phototypes III–V treated with a fractional laser (Fraxel; Reliant Technologies, Palo Alto, CA) for four to six sessions, 1–2 weeks apart [11]. None of the patients were pretreated with hydroquinone. The authors found that six out of the ten patients had 75–100 % clearing of melasma based on clinical evaluation and 30 % had less than 25 % improvement. The nonresponders were all Hispanic patients. There was a 10 % risk of post-inflammatory hypopigmentation. The risk of delayed PIH and relapse were not assessed (level of evidence, II-iii).
However, the incidence of post-inflammatory pigmentation (Fig. 16.3) following fractional laser resurfacing in Asians is high ranging from 10 to 90 % [12]. It is likely that those with melasma will experience higher risk of PIH. Hence such modality of treatment is not suitable for Asian melasma patients especially those with darker skin type.
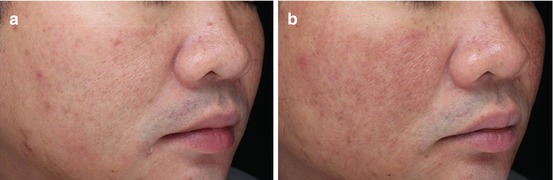
Fig. 16.3
PIH following a single treatment with the non-ablative fractional laser treatment for melasma (Photographs courtesy of National Skin Centre, Singapore)
Another study looked at the histopathologic effects of fractional laser technology on melasma. The study failed to support the efficaciousness of fractional laser resurfacing for melasma [13]. The authors treated ten patients with epidermal melasma who had Fitzpatrick skin phototypes III–IV every 2 weeks for four sessions. Biopsy specimens were obtained before treatment and 3 months after the final treatment. Sunscreen use was advocated but depigmenting agents were avoided. After treatment, lesional skin showed a decrease in the number of epidermal melanocytes and fewer enlarged melanocytes on electron microscopy; however, there was no correlation between histologic improvement and investigator-rated improvement.
Several later studies also reported lack of efficaciousness of fractional lasers for melasma. Lee et al. reported 25 melasma patients who received four monthly fractional laser treatments who achieved reduction of mean MASI score from 7.6 to 6.2. There was 60 % improvement at 4 weeks after treatment which deteriorated to 52 % at 24 weeks after treatment. Mean melanin index decreased significantly after the first two sessions, but it relapsed in subsequent follow-ups. The treatment did not alter skin elasticity. Hyperpigmentation was observed in three of 23 subjects (13 %). The authors concluded that fractional laser treatment of melasma led to some clinical improvements, but it was not as efficacious as previously reported. They recommend judicious use of fractional laser for melasma in Asian skin because of its limited efficacy. There is also risk of PIH [14].
Wind et al. treated 29 melasma patients with a split-face study using four to five treatments with non-ablative 1550-nm fractional laser on half the face compared to daily topical triple combination therapy (hydroquinone 5 %, tretinoin 0.05 %, triamcinolone acetonide 0.1 % cream) alone on the other half in a 15-week study. After the last treatment session, patients were asked to apply the triple combination cream twice weekly on both sides of the face during follow-up. Mean patient global assessment and satisfaction were significantly lower at the fractional laser-treated side (p < 0.001). Physician global assessment, melanin index, and L-value showed a significant worsening of hyperpigmentation at the fractional laser-treated side. At the triple cream-treated side, no significant change was observed. At 6-month follow-up, most patients preferred the triple cream treatment. Side effects of the fractional laser-treated side were erythema, burning sensation, edema, and pain. Nine patients (31 %) developed PIH after two or more laser sessions. The authors concluded that given the high rate of PIH, non-ablative 1550-nm fractional laser at 15 mJ/microbeam is not recommendable in the treatment of melasma. Triple cream treatment remains the gold standard treatment [15].
Subsequently, the same group of authors reported a somewhat similar study in 2011. Twenty female patients with moderate to severe melasma and Fitzpatrick skin phototypes II–V were treated either with non-ablative fractional laser therapy or triple topical therapy (hydroquinone 5 %, tretinoin 0.05 %, and triamcinolone acetonide 0.1 % cream) once daily for 8 weeks in a randomized controlled observer-blinded study. Laser treatment was performed every 2 weeks for a total of four times. Physician global assessment improved (p < .001) in both groups at 3 weeks. There was no difference in physician global assessment between the two groups. Mean treatment satisfaction and recommendation were significantly higher in the laser group at 3 weeks (p < .05). However, melasma recurred in five patients in both groups after 6 months. Side effects in the laser group were erythema, burning sensation, facial edema, and pain; in the triple topical therapy group, side effects were erythema, burning, and scaling. The authors concluded that non-ablative fractional laser therapy is safe and comparable in efficacy and recurrence rate with the triple topical therapy. It may be a useful alternative treatment option for melasma when topical bleaching is ineffective or not tolerated [16].
Fractional laser appears to show satisfactory results for melasma in Caucasians with lighter skin type but is associated with unacceptable PIH and relapses in Asians with darker skin types. It is at most equivalent to topical triple cream therapy.
16.2.5 Laser Toning with QS Nd:YAG Lasers
A procedure called “laser toning” that uses a low-energy 1064-nm Q-switched Nd:YAG laser was recently introduced for the treatment of melasma, demonstrating good results (Fig. 16.4). The procedure involves using the QS Nd:YAG laser setting at large spot size of 6 mm or 8 mm, with fluence of 2–3 J/cm2 and 1–2 J/cm2, respectively, and waving the laser beam on the surface of melasma lesions for 5–10 passes. The procedure is carried out once a week or fortnightly. The proposed mechanism of action of laser toning is subcellular selective photothermolysis of melanosomes and not melanocytes. It is speculated that melanocytes survived but the melanogenic activity downregulated such that they did not produce fully matured melanosomes [17].
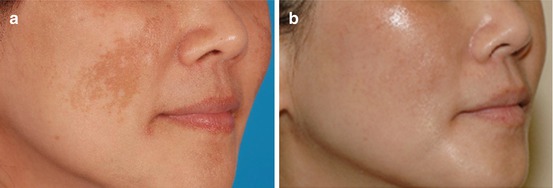
Fig. 16.4
Good improvement of melasma following eight treatments of laser toning with the QS Nd:YAG 1064-nm laser performed every 2 weeks. Fluence was 2.5 J/cm2, 6 mm spot size, 5 ns pulsed duration. Recurrence appeared 3 months after cessation of treatment (Photographs courtesy of National Skin Centre, Singapore)
There have been numerous reports of “laser toning” using the QS Nd:YAG laser. The initial reports generally concluded that the 1064-nm Q-switched Nd:YAG laser is a safe and effective modality for treating melasma in Asian patients [18–21].
A recent study comparing “laser toning” with hydroquinone and hydroquinone alone confirmed the efficacy of the treatment. Twenty-two Thai patients on split-face randomized study, combination of low-fluence QS Nd:YAG laser + 2 % hydroquinone versus topical treatment only, showed that the laser-treated side achieved 92.5 % improvement in relative lightness index and 75.9 % improvement in mMASI score, against 19.7 % and 24 %, respectively, on the topical HQ alone side (p < .001). However, the report indicated that “laser toning” procedure was associated with side effects including mottled hypopigmentation in three patients (14 %) and rebound hyperpigmentation in four (18 %) at 12-week follow-up. Melasma relapse is the rule upon cessation of treatment. Their conclusions were that QS Nd:YAG laser treatment (“laser toning”) for melasma in Asians produced only temporary improvement and had side effects. Common complications were hypopigmentation, melasma recurrence, and rebound hyperpigmentation [22]. Hypomelanosis following “laser toning” with QS Nd:YAG laser is a serious complication (Fig. 16.5). There have been several reports on this difficult to treat complication which may last several years [23–25].

Fig. 16.5
Guttate hypomelanotic macules following too frequent and high-dose laser toning with the QS Nd:YAG 1064-nm laser for melasma (Photograph courtesy of National Skin Centre, Singapore)
“Laser toning” appears to be a useful adjunct to topical treatment for melasma. But it should be used with caution. The laser physician should use conservative treatment protocol when carrying out “laser toning.” Generally, the frequency of “laser toning” should not exceed more often than once fortnightly, and the fluence should be kept low. “Laser toning” should be stopped at the earliest indication of guttate hypomelanotic macules appearing.
16.2.6 Intense Pulsed Light
Intense pulsed light (IPL) is a broadband light source and is not a laser device. The IPL emits light of wavelength stretching from 500 to 1200 nm. This spectrum of wavelength falls within the absorption spectrum of melanin and oxyhemoglobin. Hence, it can be used to treat superficial pigmentary lesions including melasma. “Cutoff” filters can be placed across IPL sources to eliminate unwanted shorter wavelengths to prevent epidermal burn. These filters are especially useful when using IPL on darker skin type.
Several studies have reported improvements of melasma with IPL with minimal side effects. But patients often require multiple treatments (Fig. 16.6).
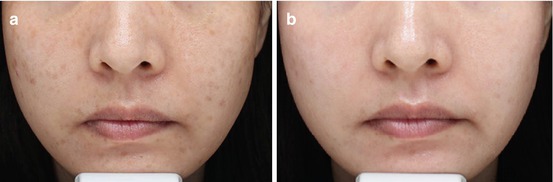
Fig. 16.6
Fairly good response of melasma to six sessions at monthly interval of IPL
A report from Taiwan compared IPL treatment with HQ against HQ alone on 33 patients with Fitzpatrick skin phototypes III and IV having mixed melasma. Patients received four monthly sessions of IPL. Using the mexameter, the authors calculated a relative melanin index (defined as the difference between the melanin index of lesional skin and the melanin index of normal skin). In the IPL/HQ group (17 females), 35 % had greater than 50 % improvement compared to the HQ-alone group (16 control) with only 14 % experiencing greater than 50 % improvement. The patients who received IPL treatment had a 39.8 % decrease in the relative melanin index after four treatments (16 weeks), while the control group receiving topical therapy alone had only an 11.6 % decrease. At 24-week posttreatment, the improvement on the IPL-treated side had decreased less to a mean of 24.2 %, suggesting the need for maintenance treatments. Side effects of the IPL included some crusting lasting for 1–2 weeks; transient PIH seen in 12 % was resolved with the use of HQ [26].
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


