This section is dedicated to the comprehensive evaluation of the overhead throwing athlete’s elbow. The elbow provides a unique diagnostic dilemma that requires extensive knowledge and appreciation of elbow anatomy and kinematics, given the extreme forces seen across the elbow during the overhead throwing motion, the superficial nature of the majority of anatomic structures, and the complex interplay among bony, ligamentous, musculotendinous, and neurologic structures. The physical examination of the ulnar collateral ligament, valgus extension overload syndrome, medial and lateral epicondylitis, posterolateral rotatory instability, tendon ruptures, and compressive neuropathies will be covered.
Key points
- •
The examination of the elbow in throwing athletes is catered to the superficial anatomic structures and extreme forces through the joint and a proper physical examination is critical as imaging of the athlete’s elbow is often abnormal.
- •
The major focus of the physical examination is on the medial elbow, primarily on the ulnar collateral ligament (UCL), medial epicondylitis, ulnar nerve, and posteromedial impingement in valgus extension overload syndrome.
- •
UCL pathology and medial epicondylitis both have a high incidence of ulnar nerve compression at the elbow, which must be examined for neurologic deficits and instability.
- •
The anterior and lateral elbow should not be neglected, as lateral epicondylitis and biceps tendon pathologies can also occur in throwers.
- •
Rare peripheral nerve compression syndromes should remain in the differential, and the examiner should understand the nuances between proximal median nerve entrapment, anterior interosseous nerve syndrome, posterior interosseous nerve syndrome, radial tunnel syndrome, and Wartenberg’s syndrome.
Introduction
The throwing athlete’s elbow provides a unique diagnostic dilemma that requires extensive knowledge and appreciation of elbow anatomy and kinematics, given the extreme forces seen across the elbow during the overhead throwing motion, the superficial nature of the majority of anatomic structures, and the complex interplay among bony, ligamentous, musculotendinous, and neurologic structures. The physical examination (PE) of the elbow is of critical importance given the increased accuracy of some tests compared to advanced imaging, and the clinical diagnosis of several pathologies.
The examination of the throwing elbow
The Basics
The examination of the throwing elbow is often less commonly seen by most orthopedists, but an understanding of anatomy and throwing mechanism can guide the examiner through the PE given the superficial nature of the majority of elbow structures. Throwing imposes extremely high valgus stresses (nearly 60–65 Nm) across the elbow, primarily during the late cocking and early acceleration phases of throwing, which generates tension through the medial elbow, compression on the lateral elbow, and shear forces on the posterior elbow structures creating predictable injury patterns that should be systematically investigated. As with the shoulder, the cervical spine, joint above (shoulder–covered previously), and below (the wrist) should be examined to rule out concomitant pathologies.
Inspection and Palpation
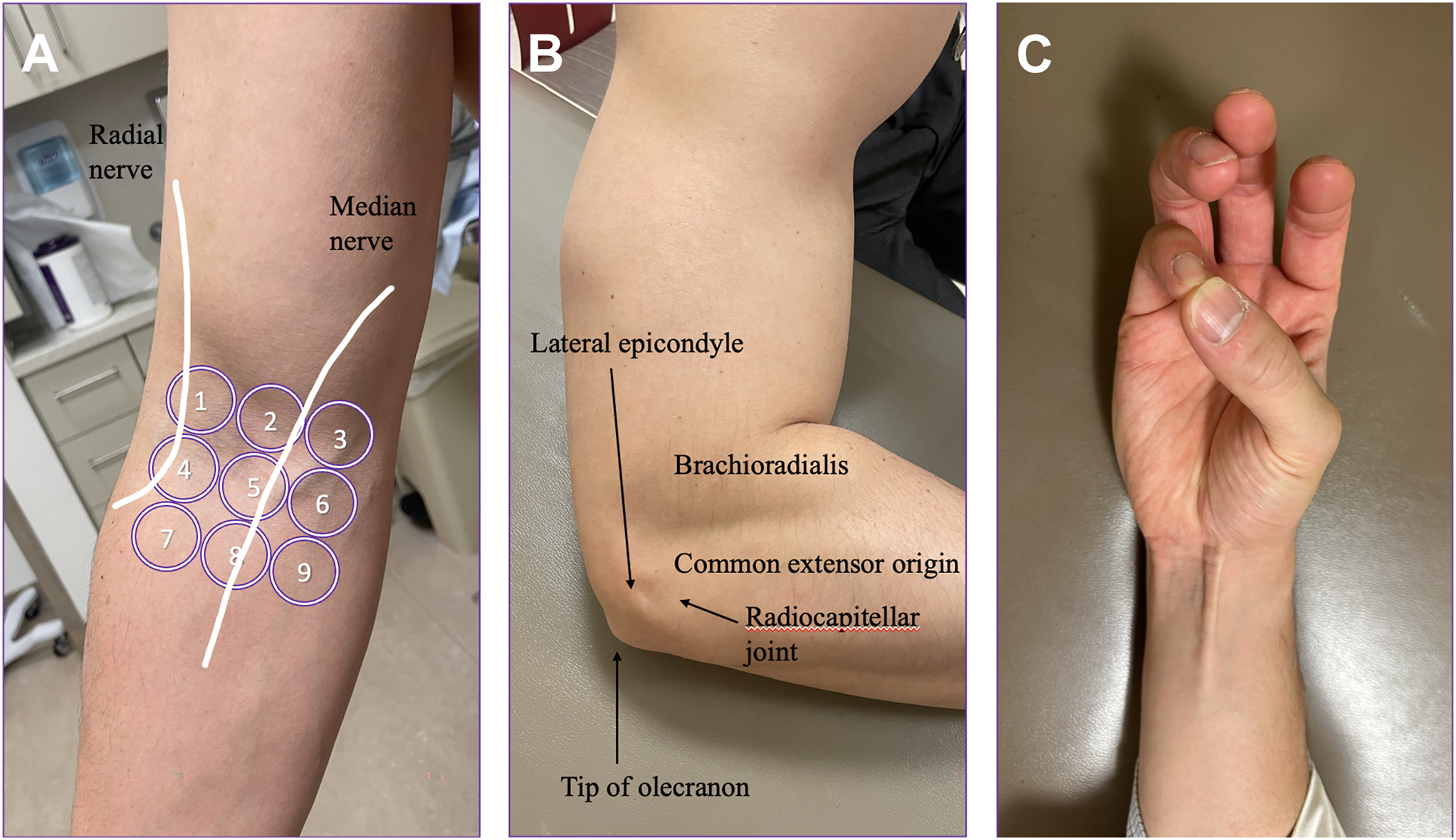
Initial examination of the elbow begins with inspection of the resting position carrying angle, which ranges from normal values of 11° to 14° of valgus in men and from 13° to 16° in women. , In young pitchers especially, increased repetitive stresses from repetitive overhead throwing can lead to increased carrying angles, which has not been found to correlate with injury risk. In addition, patients with flexion contractures can have falsely decreased carrying angles as the elbow becomes more varus with increasing elbow flexion. Palpation of the elbow should be performed systematically to avoid misdiagnoses. As the patient is usually seated in an examination room, for convenience, the authors prefer to start anteriorly and work their way lateral, posterior, and then medial. Anteriorly the biceps tendon, lacertus fibrosis, and radial and median nerve courses can be palpated according to the rule-of-nine test developed by Loh and colleagues for radial tunnel syndrome ( Fig. 1 A ). , Laterally, an effusion can be palpated in the triangular anconeus “soft spot” between the lateral epicondyle, radial head, and olecranon tip and is often accompanied by a resting elbow position of 70° to 80°, which maximizes capsular volume. The lateral epicondyle, radial head, lateral ulnar collateral ligament (UCL), extensor carpi radialis brevis (ECRB), and posterolateral olecranon can all be easily palpated for tenderness given the superficial nature of these landmarks ( Fig. 1 B). Of particular important in throwers is tenderness over the radial head as valgus extension overload (VEO) can lead to cartilage wear in this portion of the elbow. With a slight valgus load and palpation of the radiocapitellar joint, pain, crepitus, or snapping can be felt in cases of capitellar osteochondritis dissecans (OCD) in adolescents or posterolateral plica in adults. , Posteriorly, palpation is focused on the triceps tendon and olecranon. The triceps tendon insertion for tendinitis, olecranon tip for stress fracture, superficial olecranon for bursitis, and posteromedial and posterolateral olecranon with the elbow flexed to 30° to relax the triceps should be performed. Lastly, the medial elbow is palpated. The medial epicondyle and flexor pronator mass (FPM) is palpated for pain, as well as the course of the ulnar nerve posterior to the medial epicondyle, and both the ulnar nerve and medial triceps can be palpated for subluxation or snapping, respectively, across the medial epicondyle. Elbow flexion to 50° to 70° moves the FPM anterior to the UCL, making UCL palpation more accurate in the sulcus just distal to the medial epicondyle and anterior to the ulnar nerve. ,
Range of Motion, Strength, and Neurovascular Testing
The thrower’s elbow should be taken through systematic range of motion (ROM) testing and compared to the contralateral elbow. A normal extension-flexion arc is from 0° to 145°, with approximately 80° of pronation and supination. Limitations in ROM should be assessed for feel, as hard end points are likely osteophyte formation in the coronoid fossa (flexion), olecranon fossa (extension), or radiocapitellar joint (pronosupination), while soft end points are due to fibrous contractures, effusion, or diffuse synovitis. , Crepitus, locking, or catching mechanical symptoms throughout ROM can be due to plicas, unstable OCD lesions, or loose bodies. Hyperextension up to 15° can be due to ligamentous laxity, while flexion contractures are particularly common in overhead throwers, with up to 20° noted to be due to physiologic changes and a mean decrease of 5.5°±7.8° compared to the contralateral elbow in professional baseball pitchers. While historical studies note necessary functional ROM of 30° to 130° and pronosupination of 50° to 50°, recent studies with modern tasks such as keyboard and cellphone use have demonstrated increased need for pronation and flexion. , Baseball pitchers, in particular, require full supination for most breaking balls, and nearly all overhead throwing athletes require full pronation for follow-through. Strength testing should similarly be performed for flexion, extension, supination, pronation, grip, and both wrist and finger flexion and extension. Given the proximity of the brachial artery and median, radial, and ulnar nerves to the elbow, a thorough neurovascular examination should always be performed, with further in-depth compressive neuropathy special testing if clinical concern arises. For the ulnar nerve, in particular, this entails a sensory examination to light touch in both the dorsal ulnar hand (dorsal sensory branch of the ulnar nerve that branches prior to Guyon’s canal), and the volar ulnar digits (ulnar nerve superficial sensory branches through Guyon’s canal), and motor testing of the fourth and fifth flexor digitorum profundus (FDP) and first dorsal interossei (pre-Guyon’s canal and post-Guyon’s canal, respectively). Lastly, special testing of specific pathologies that are near the top of the examining surgeons’ differential diagnosis should be performed, as described in later discussion.
Ulnar collateral ligament injuries
The UCL is the most commonly injured structure of the elbow and cause for missed time in professional baseball pitchers given the extreme valgus stresses through the medial elbow. , It can be either simply sprained or partially or fully torn anywhere along its course from approximately 8 mm anterior and distal to the medial epicondyle apex to its insertion approximately 6 to 8 mm distal to the ulnohumeral joint line on the sublime tubercle. , A variety of special tests have been described, and the examiner should always examine the ulnar nerve for neuropathy or subluxation, and for the presence of a palmaris longus using the Schaeffer test for possible future surgical planning ( Fig. 1 C).
Milking Maneuver
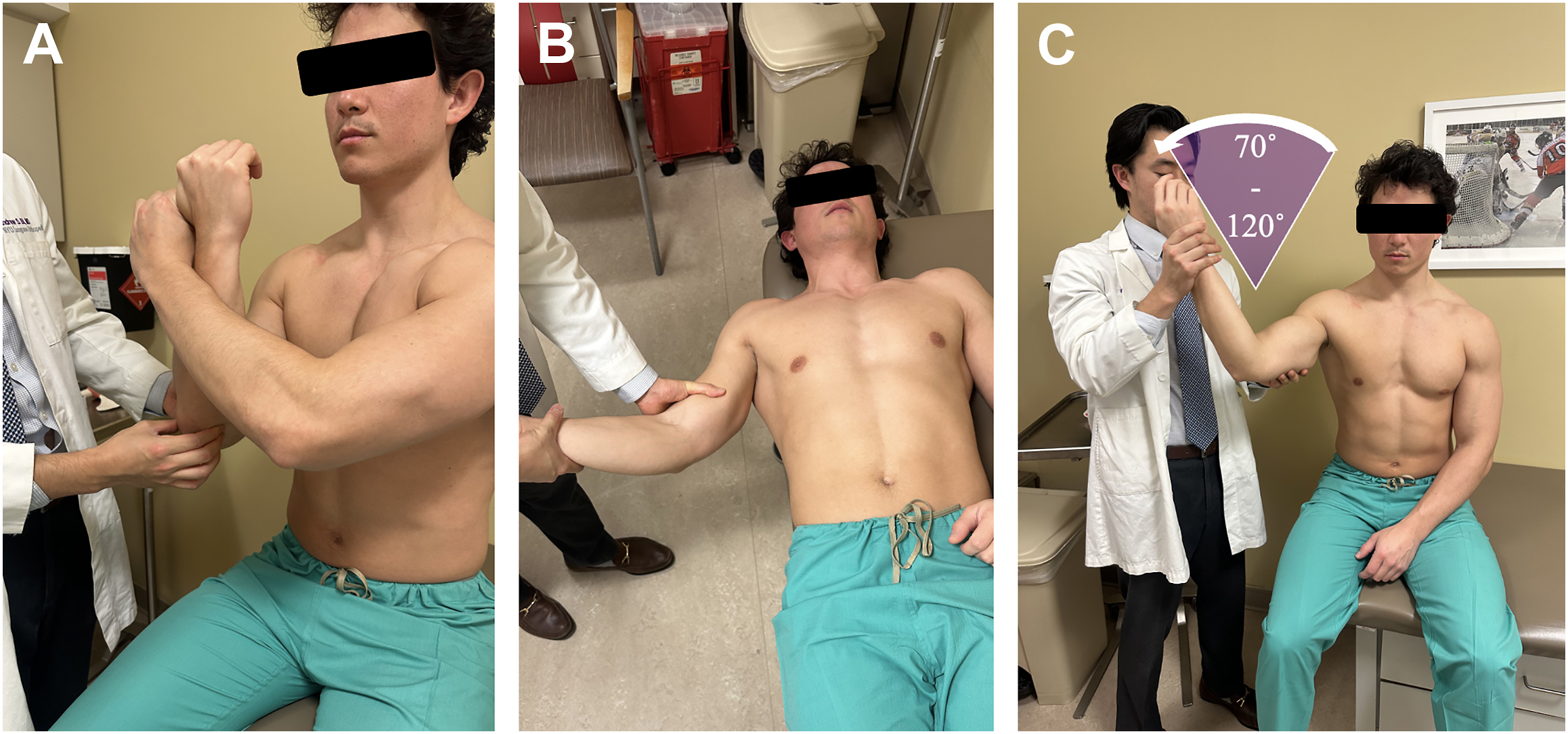
The milking maneuver was first described by Veltri and colleagues in 1994 at the American Shoulder and Elbow Surgeons’ 10th Specialty day. , The affected elbow is flexed to 90° and fully supinated, and either the examiner or the patient’s opposite hand is used to grasp the thumb of the affected hand. The examiner’s ipsilateral hand is used to palpate the UCL for both tenderness and medial joint space opening while a valgus force is applied through traction on the patient’s thumb ( Fig. 2 A ). A modification of the milking maneuver was proposed by Marc Safran in 2003 to eliminate the bony contributions to elbow stability that predominate at increasing elbow flexion angles and confounding motion of shoulder external rotation (ER), with the patient’s affected elbow at 70° flexion and their contralateral hand held under their upper arm as counter to prevent abduction and ER of the shoulder. , To our knowledge, there have been no studies evaluating the diagnostic accuracy of the milking maneuver published.
Valgus Stress Test
The classic valgus stress test for UCL injuries was published in 1981 by Norwood and colleagues, describing a new “elbow abduction stress test” in 4 patients. They described positioning the patient supine with the shoulder abducted for the evaluation “of an injured right elbow stabilize the distal humerus with the left hand. Rest your left elbow against his side for hand support and support the patient’s hand with your right hand. Gently swing the arm and stress the medial side of the elbow, much in the same manner as when doing the abduction stress test of the knee. This is performed at 15° to 20° of flexion.” Although there is some confusion with the wording, the figure demonstrates the examiner’s left hand on the patient’s lateral distal humerus without the examiner’s elbow involved, and the patient’s forearm held in full supination. The elbow flexion helps remove bony constraint by “unlocking” the olecranon tip from the olecranon fossa, and further work by O’Driscoll and colleagues has demonstrated the utility of keeping the forearm in pronation, to prevent a false positive (FP) from subtle posterolateral rotatory instability (PLRI) mimicking medial laxity ( Fig. 2 B). O’Driscoll and colleagues demonstrated sensitivity (SN) of 65% and specificity (SP) of 50% for this examination when compared to intraoperative examination of the UCL.
Moving Valgus Stress Test
Due to deficiencies in the prior examination maneuvers for detecting UCL injuries, particularly partial tears, O’Driscoll and colleagues developed the moving valgus stress test in 2005 to replicate actual stresses involved in the throwing motion. The elbow experience maximum valgus force from 120° to 90° during late cocking and early acceleration, which was the basis for the examination, in which the patient is seated or standing and the shoulder is abducted 90°. The elbow is maximally flexed, and then a valgus torque is applied to the elbow until the shoulder reaches maximal ER, then while maintaining this constant valgus torque, the elbow is quickly extended to about 30° (as expected, patients with shoulder pathology should be treated with caution with this maneuver; see Fig. 2 C). A positive test is both reproducible medial elbow pain and that the maximal pain is produced between late cocking (120° elbow flexion) and early acceleration (70° elbow flexion). This angle of maximal pain was referred to by O’Driscoll as the shear angle , and the total arc of painful motion was deemed the shear range . In the same study, they reported SN of 100% and SP of 75% compared to intraoperative assessment.
Valgus extension overload
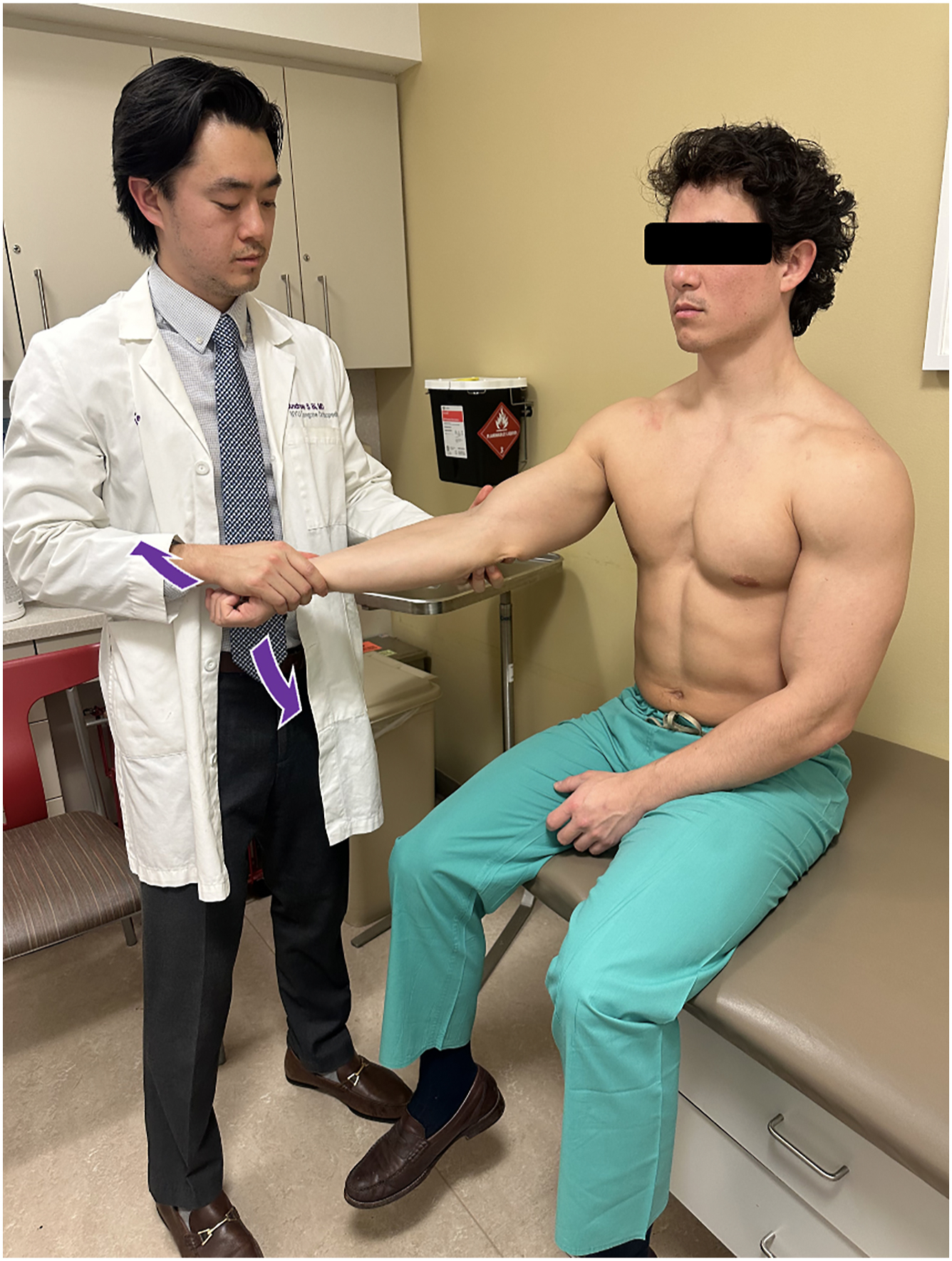
As the thrower enters the deceleration phase of throwing, especially with medial-sided elbow laxity such as above UCL pathology, the lateral side of the elbow experiences compressive forces and the posteromedial elbow experiences high shear forces across the joint. This mechanism has been coined VEO syndrome by Wilson and colleagues in 1983. , This repetitive posteromedial impingement can lead to posteromedial olecranon or trochlear spurring/osteophyte formation, which may fracture leading to loose bodies, posteromedial olecranon stress fractures, posteromedial capsular synovitis, and loss of terminal extension. , On PE, palpation of the posteromedial elbow often elicits pain at the posteromedial olecranon tip, and loss of terminal extension is common in ROM testing. Pain with forced elbow extension is the basis of the VEO test, or extension impingement test, which is performed with the patient seated and shoulder slightly FF. A bounce test for a posteromedial osteophyte can also be performed where the elbow is repeatedly forced into full extension by the examiner while applying a valgus stress, with a positive result indicated by reproducible posteromedial elbow pain as the medial tip of the olecranon impinges on the medial wall of the olecranon fossa ( Fig. 3 ). ,
Related posts:
 Evaluation and Preparation of the Baseball Player in the Athletic Training Room
Evaluation and Preparation of the Baseball Player in the Athletic Training Room
 In Season Return to Play Issues for the Baseball Player
In Season Return to Play Issues for the Baseball Player
 The Physical Examination of the Throwing Shoulder
Superior Labrum Anterior to Posterior Lesions and Capsular Injuries in the Throwing Athlete
The Physical Examination of the Throwing Shoulder
Superior Labrum Anterior to Posterior Lesions and Capsular Injuries in the Throwing Athlete
 Custom Craniofacial Implants
Custom Craniofacial Implants
 Lips and Chin
Lips and Chin
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


