Marko Godina in his landmark paper in 1986 established the principle of early flap coverage for reconstruction of traumatic lower extremity injuries to minimize edema, fibrosis, and infection while optimizing outcomes. However, with the evolution of microsurgery and wound management, there is emerging evidence that timing of reconstruction is not as critical as once believed. Multidisciplinary care with a combined orthopedic and reconstructive approach is more critical for timely and appropriate definite treatment for severe lower extremity injuries.
Key points
- •
Although early reconstruction within 72 hours of injury has long been held as the gold standard for treating traumatic lower extremity injuries, recent evidence suggests this ideal window can likely be extended 1 to 2 weeks.
- •
Advances in local wound care, particularly negative pressure wound therapy, have allowed for successfully temporizing lower extremity wounds.
- •
Although timing of reconstruction may be less important than previously suggested, expeditious treatment using a multidisciplinary approach remains the ultimate goal.
Introduction
Lower extremity reconstruction, particularly in the setting of trauma, remains one of the most challenging tasks for the plastic surgeon. Relevant factors to consider include bony restoration, flap choice, and timing. Considerable debate has continued regarding the ideal timing of reconstruction for lower extremity trauma. For nearly 3 decades, early reconstruction within 72 hours of injury has been considered the gold standard. However, with the evolution of microsurgical practices and new advances in wound care, specifically negative pressure wound therapy (NPWT), there has been a paradigm shift in the timing for managing these injuries.
Evidence for early timing of reconstruction
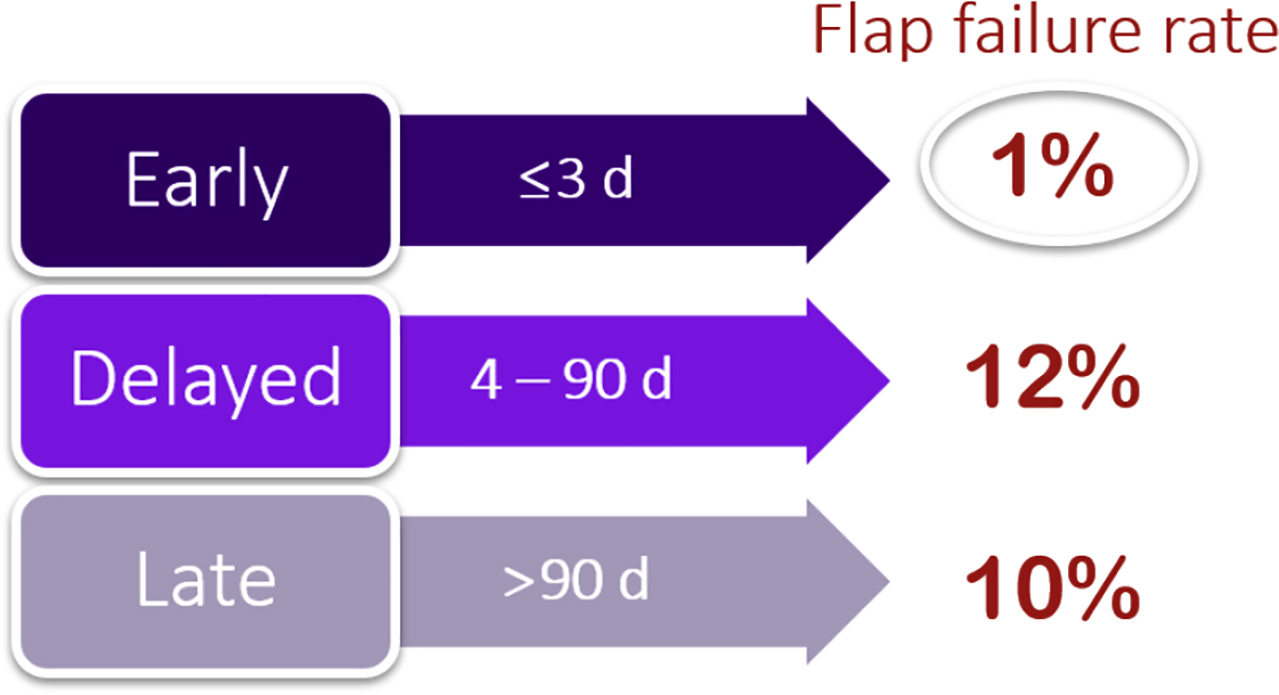
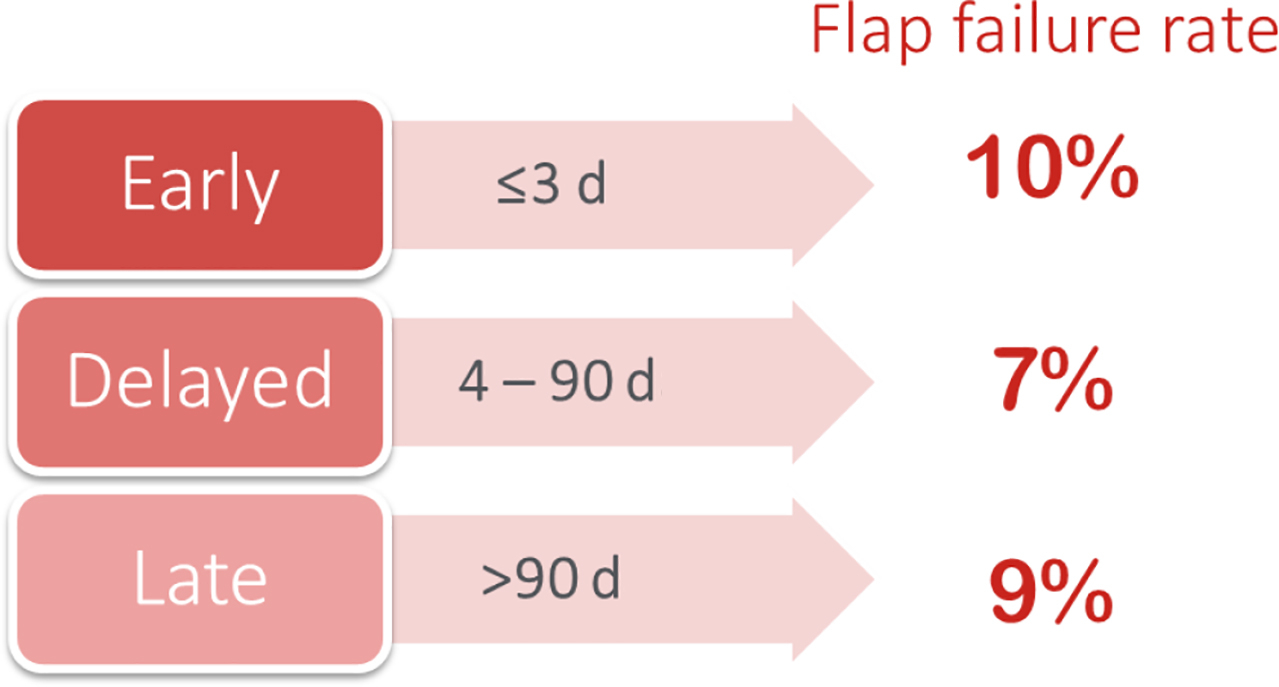
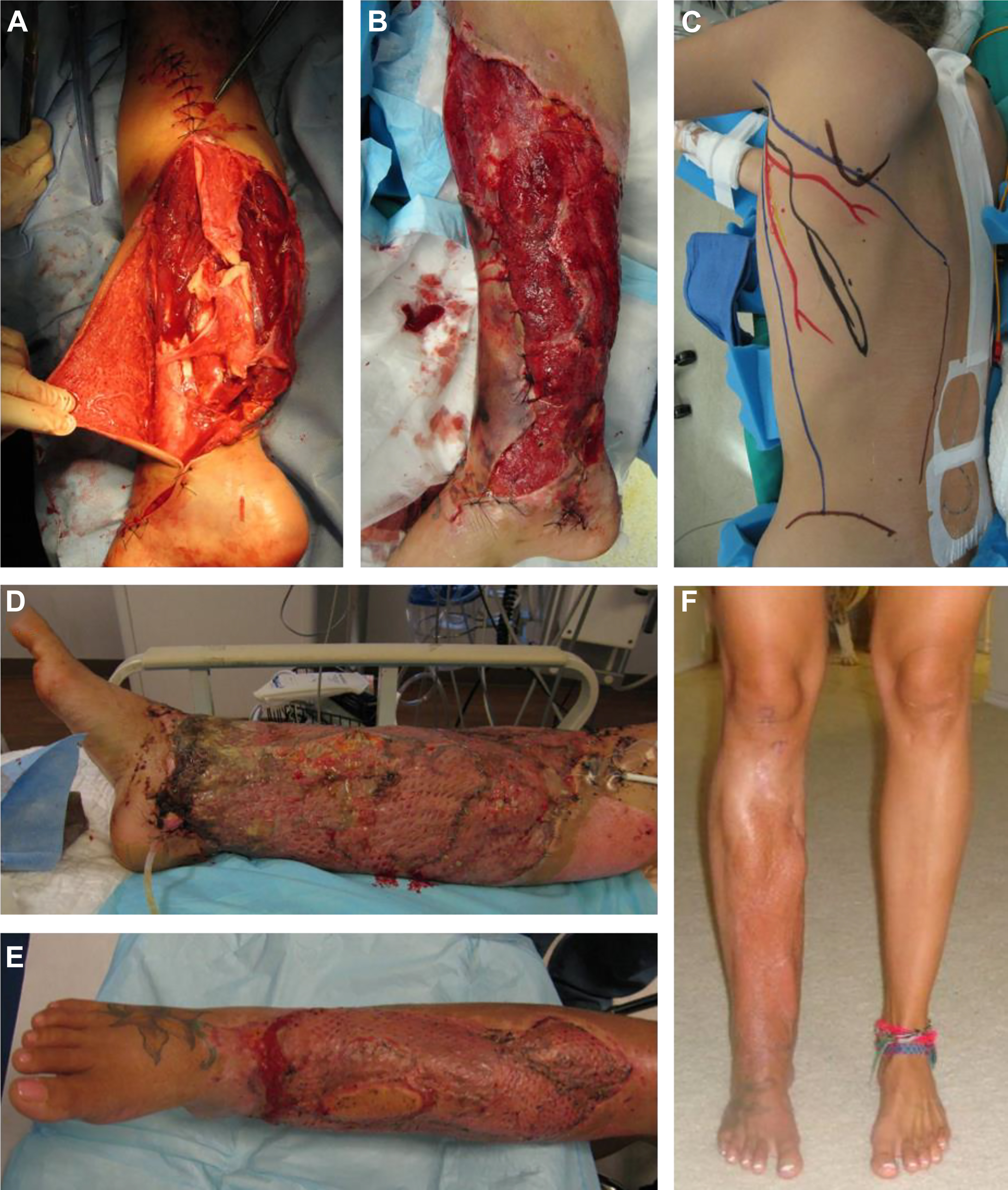
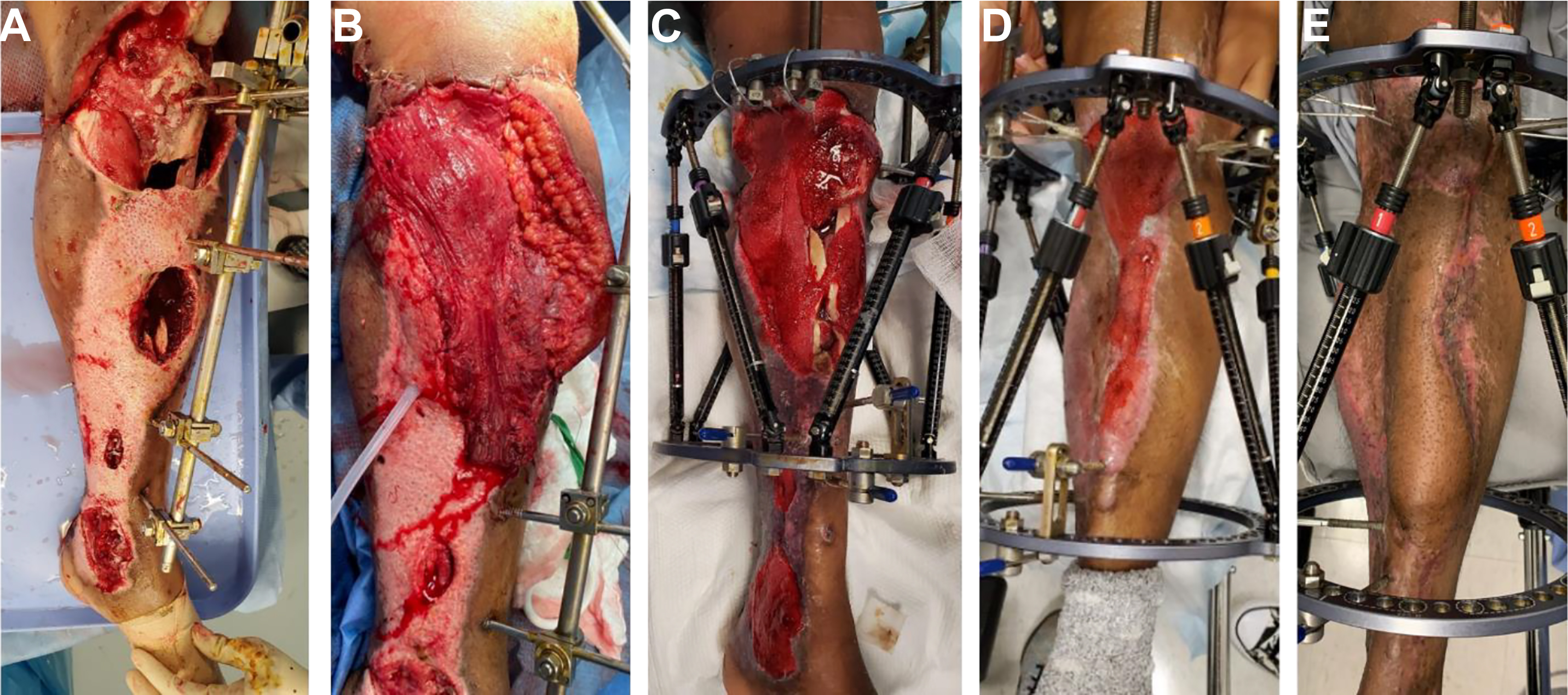
In 1986, Marko Godina’s landmark paper “Early Microsurgical Reconstruction of Complex Trauma of the Extremities” provided evidence for the benefits of free flap coverage within 72 hours from initial injury. His large series of over 500 patients demonstrated lower rates of flap failure and postoperative infection in the early group compared with flaps performed after 72 hours ( Figs. 1–5 ). The tenet of early reconstruction in lower extremity trauma came to be accepted as the relative gold standard as subsequent studies provided further corroboration. However, although Godina’s original work established some of the guiding principles for free flap reconstruction in lower extremity trauma, there were some limitations. Most notably, his analysis did not control for the learning curve that occurred over time: his first 100 cases had a flap failure rate of 26% compared with only 4% in his last 100 cases, and most of his initial 100 cases were performed in a delayed fashion. Despite this confounding factor, the concept of early coverage within 3 days of injury became the standard of care, especially given the rationale of less scarring and fibrosis in the immediate stages after injury. Furthermore, it has been well documented that the onset of significant inflammation in the delayed period after injury can affect all tissue types of the lower extremity, from the skin and muscle to the neurovascular structures, resulting in compromised outcomes after free flap reconstruction.
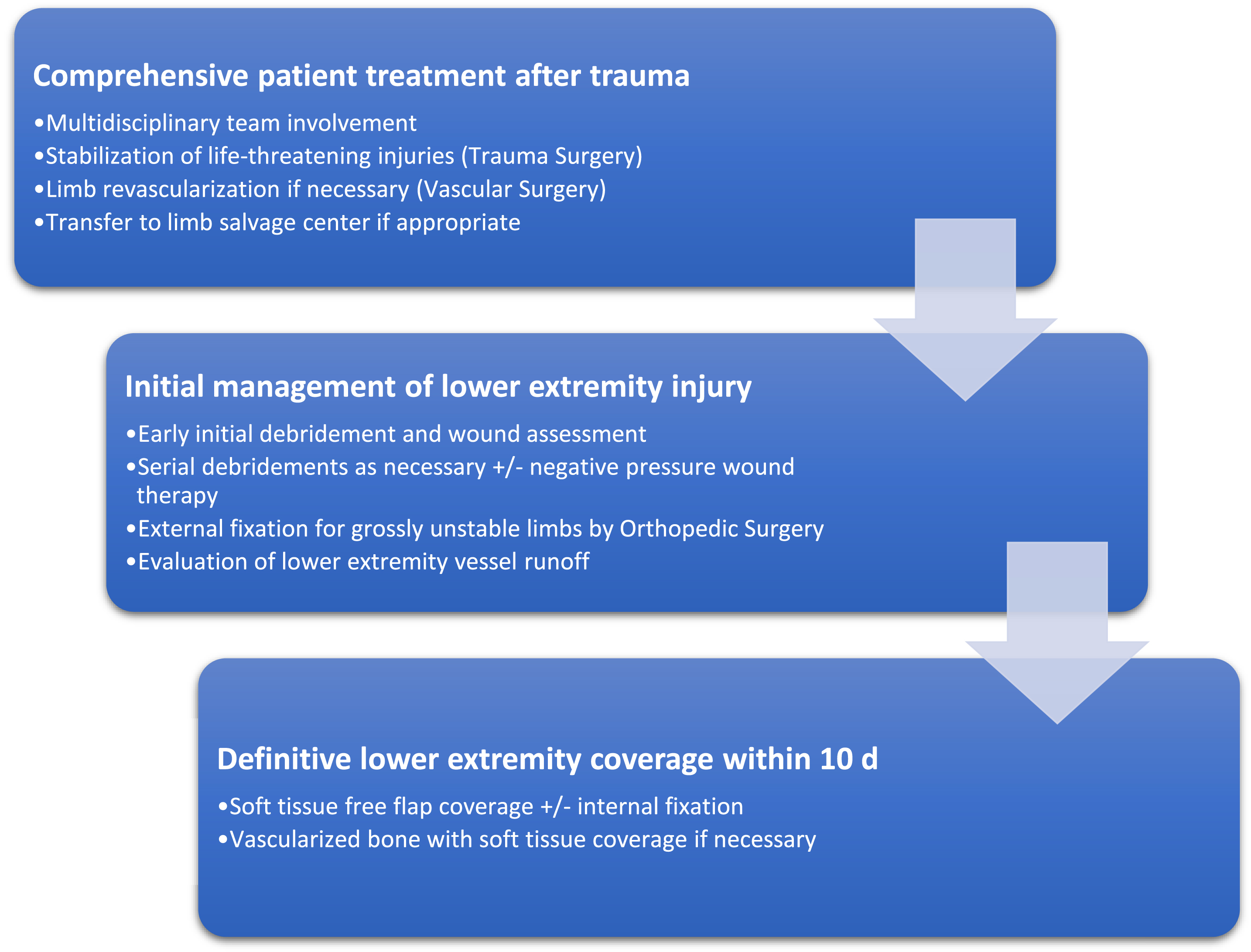
With the development of regional trauma centers specializing in limb salvage, treatment of severe lower extremity injuries has become standardized with a multidisciplinary approach involving vascular, orthopedic, and plastic surgeons. Open fractures are debrided early and fixated either with temporary external fixators or internal fixation, followed by stable soft tissue coverage, usually in the form of free tissue transfer. However, delays in flap coverage can occur because of delay in referral to a tertiary trauma center, other life-threatening injuries, or attempts at wound closure with skin grafts or local flaps. Given these practical limitations and the arbitrary nature of Godina’s original timing groups, several additional studies have investigated the impact of timing on outcomes after free flap reconstruction of the lower extremity and whether this early safe period of 3 days can be extended ( Table 1 ). ,
| Author, Year | Study Design (# of Patients) | Outcomes Assessed | Reconstruction Criteria | Timing Windows | Conclusion |
|---|---|---|---|---|---|
| Byrd et al, 1985 | Prospective (n = 191) | Flap failure Amputation rate Osteomyelitis Time to bony union Length of stay Time to closure | Open tibial fractures (type I-IV) | Acute 1-5 d Subacute 1-6 w Chronic >6 w | Acute best for all outcomes |
| Godina et al, 1986 | Retrospective (n = 532) | Flap failure Infections Time to bony union Length of stay | Lower extremity trauma | Early <72 h Delayed 72 h-3 mo Late >3 mo | Acute best for all outcomes |
| Francel et al, 1992 | Retrospective (n = 72) | Flap failure Reoperations Osteomyelitis SSI Length of stay (LOS) Time to bony union | Gustilo IIIB injuries | <15 d 15–30 d >30 d | <15 d group: Fewer flap failures and reoperations, decreased LOS and time to bony union |
| Kolker et al, 1997 | Retrospective (n = 451) | Flap failure Reoperation | Below knee injuries | Acute <22 d Subacute 22–60 d Chronic >60 d | No difference in outcomes |
| Karanas et al, 2008 | Retrospective (n = 14) | Flap failure Osteomyelitis | Lower extremity trauma | All >72 h | No flap loss in 14 patients |
| Hill et al, 2012 | Retrospective (n = 60) | Flap failure Reoperation SSI | Lower extremity trauma | <30 d 31–90 d >91 d | No significant difference in outcomes Trend toward lower rates of failure among >91 d group |
| Raju et al, 2014 | Retrospective (n = 50) | Flap failure Reoperation Infection | Lower extremity trauma (All received NPWT prior to flap) | 1 wk 2 wk 3 wk 4 wk 5 wk 6 wk 7 wk | No difference in outcomes |
| Bellidenty et al, 2014 | Retrospective (n = 89) | Flap failure Osteomyelitis | Lower extremity trauma Gustilo 3B injuries (emergency vs delayed cases referred to center for coverage) | Emergency Delayed | Lower failure and infection rates in ‘emergency’ group, increased in delayed group |
| Starnes-Roubaud et al, 2015 | Retrospective (n = 51) | Flap failure Osteomyelitis Bony union Ambulation | Lower extremity trauma | <15 d >15 d | No difference in outcomes |
| Lee et al, 2018 | Retrospective (n = 358) | Flap failure Return to OR | Lower extremity trauma | 0–3 d 3–9 d 10–90 d >90 d | No difference in outcomes between 0–3 and 3–9 d; higher complications for 10–90 d |
Related posts:
 Propeller Flaps in Lower Extremity Reconstruction
Propeller Flaps in Lower Extremity Reconstruction
 The Medial Sural Artery Perforator Flap in Lower Extremity Reconstruction
The Medial Sural Artery Perforator Flap in Lower Extremity Reconstruction
 Free-Style Free Perforator Flaps in Lower Extremity Reconstruction
Free-Style Free Perforator Flaps in Lower Extremity Reconstruction
 Orthoplastic Approach to Lower Extremity Reconstruction
Orthoplastic Approach to Lower Extremity Reconstruction
 The Anterolateral Thigh Perforator Flap
The Anterolateral Thigh Perforator Flap
 Lower Extremity Reconstruction in the Pediatric Population
Lower Extremity Reconstruction in the Pediatric Population
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


