Fig. 2.1
Illustration of the difference between uniform shear and surface divergence. (a) Uniform, high-shear stress, no divergence, and thus no stretch of the cell surface; (b) high rate of positive divergence (as well as shear stress), cell/cell membrane in stretch-activated state; (c) high rate of negative divergence (as well as shear stress), cell/cell membrane compressed together (This figure is reproduced with permission from Collis et al. 2010)
Bubbles can also grow slowly due to asymmetric gas flow during stable cavitation, and this interesting phenomenon is called rectified diffusion. While a bubble is expanded in the ultrasound field, the surface area and the internal volume of the bubble increase, but thickness of bubble shell decreases. Due to the increased volume, the internal gas density will decrease so that the dissolved gas in surrounding liquid can flow into the bubble. The opposite directional gas flow can happen during the period of compressional ultrasound field. However, the inflow and the outflow of gas are asymmetric since the surface area and the gas pressure gradient at each stage are different. In other words, the surface area of bubble and the gas pressure gradient are greatest at the peak of expansion, so that gas inflow will be maximum. But outflow will be much smaller due to the minimized surface area and low gas pressure gradient due to thickened bubble shell. Harvey et al. suggested rectified diffusion during the study of the formation of bubbles in animals, and Crum estimated the minimally required external pressure to be 0.01 MPa in water (Harvey et al. 1944; Crum 1984). Lavon et al. suggested that rectified diffusion in intercellular lipid layers can be the main mechanism of sonophoresis (Lavon et al. 2007).
2.2.2.2 Inertial Cavitation
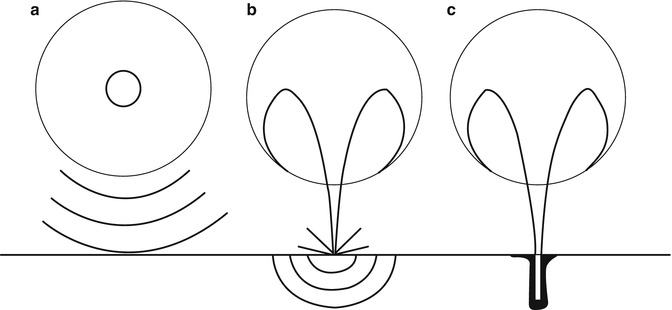
Inertial cavitation corresponds to the violent growth and collapse of bubbles that can occur within a period of a single cycle or a few cycles, depending on acoustic pressure as well as frequency and size distribution of bubbles associated with resonant frequency (Mitragotri et al. 1996; Suslick 1989; Colussi et al. 1998). Apfel and Holland derived a mechanical index (MI), which represents the likelihood that inertial cavitation will occur for medical ultrasound imaging systems (Apfel et al. 1991). The organizations such as the American Institute of Ultrasound in Medicine (AIUM), National Electrical Manufacturers Association (NEMA), and Food and Drug Administration (FDA) have adopted an MI, weighted for the frequency response, of ![$$ {I}_{\mathrm{MI}}={P}_{\mathrm{neg}}\left[\mathrm{Mpa}\right]/\sqrt{f_0}\left[\mathrm{MHz}\right] $$](http://plasticsurgerykey.com/wp-content/uploads/2017/10/A309386_1_En_2_Chapter_IEq1.gif) (P neg, maximum negative pressure, f 0, frequency). The likelihood of inertial cavitation increases with decreasing frequency and lowering peak-negative pressure (Meltzer 1996). For inertial cavitation, lower frequencies give bubbles more time to grow in the expansion cycle (the rapid expansion of gaseous bubbles) and consequently produce more violent collapse during the compression cycle (the collapse of gaseous bubbles). Violent collapse of cavitation bubbles might either generate shock waves in the bulk of the liquid or a micro-jet which is from the asymmetric collapse of bubbles inducing fissures on membranes near a boundary. Figure 2.2 schematically shows the shock wave and micro-jet produced by inertial cavitation events. A spherical collapse of a bubble yields high-pressure cores that emit shock waves with amplitudes exceeding 10 kbar (Pecha and Gompf 2000). The disruption of a target exposed to such a pressure wave may occur through relative particle displacement, compressive failure, tensile stress, or shear strain (Lokhandwalla and Sturtevant 2000). When a bubble collapses asymmetrically near a boundary, it generally produces a well-defined high-velocity micro-jet (Katz 1995; Popinet and Zaleski 2002). Micro-jet distortion of bubble collapse depends on the surface of the bubble encounters. If the surface is larger than the resonant size of the bubble (diameter of 1 ~ 100um at 20 ~ 500 kHz (Leighton 1997)), the resulting collapse will be in micro-jet form (see Fig. 2.2) (Tezel et al. 2003).
(P neg, maximum negative pressure, f 0, frequency). The likelihood of inertial cavitation increases with decreasing frequency and lowering peak-negative pressure (Meltzer 1996). For inertial cavitation, lower frequencies give bubbles more time to grow in the expansion cycle (the rapid expansion of gaseous bubbles) and consequently produce more violent collapse during the compression cycle (the collapse of gaseous bubbles). Violent collapse of cavitation bubbles might either generate shock waves in the bulk of the liquid or a micro-jet which is from the asymmetric collapse of bubbles inducing fissures on membranes near a boundary. Figure 2.2 schematically shows the shock wave and micro-jet produced by inertial cavitation events. A spherical collapse of a bubble yields high-pressure cores that emit shock waves with amplitudes exceeding 10 kbar (Pecha and Gompf 2000). The disruption of a target exposed to such a pressure wave may occur through relative particle displacement, compressive failure, tensile stress, or shear strain (Lokhandwalla and Sturtevant 2000). When a bubble collapses asymmetrically near a boundary, it generally produces a well-defined high-velocity micro-jet (Katz 1995; Popinet and Zaleski 2002). Micro-jet distortion of bubble collapse depends on the surface of the bubble encounters. If the surface is larger than the resonant size of the bubble (diameter of 1 ~ 100um at 20 ~ 500 kHz (Leighton 1997)), the resulting collapse will be in micro-jet form (see Fig. 2.2) (Tezel et al. 2003).
(P neg, maximum negative pressure, f 0, frequency). The likelihood of inertial cavitation increases with decreasing frequency and lowering peak-negative pressure (Meltzer 1996). For inertial cavitation, lower frequencies give bubbles more time to grow in the expansion cycle (the rapid expansion of gaseous bubbles) and consequently produce more violent collapse during the compression cycle (the collapse of gaseous bubbles). Violent collapse of cavitation bubbles might either generate shock waves in the bulk of the liquid or a micro-jet which is from the asymmetric collapse of bubbles inducing fissures on membranes near a boundary. Figure 2.2 schematically shows the shock wave and micro-jet produced by inertial cavitation events. A spherical collapse of a bubble yields high-pressure cores that emit shock waves with amplitudes exceeding 10 kbar (Pecha and Gompf 2000). The disruption of a target exposed to such a pressure wave may occur through relative particle displacement, compressive failure, tensile stress, or shear strain (Lokhandwalla and Sturtevant 2000). When a bubble collapses asymmetrically near a boundary, it generally produces a well-defined high-velocity micro-jet (Katz 1995; Popinet and Zaleski 2002). Micro-jet distortion of bubble collapse depends on the surface of the bubble encounters. If the surface is larger than the resonant size of the bubble (diameter of 1 ~ 100um at 20 ~ 500 kHz (Leighton 1997)), the resulting collapse will be in micro-jet form (see Fig. 2.2) (Tezel et al. 2003).Fig. 2.2
Three possible modes through which inertial cavitation may enhance SC permeability: (a) spherical collapse near the SC surface emits shock waves, (b) impact of an acoustic micro-jet on the SC surface, and (c) micro-jet physically penetrates into the SC (The figure is reproduced with permission from Tezel et al. 2003)
Shock waves generated by inertial cavitation can cause structural alteration in the surrounding corneocyte lipid interface regions. Because channels for diffusion could be newly formed between keratinocyte-lipid interfaces, drugs can be delivered through these aqueous channels which are formed within the disordered lipid bilayers of SC. Furthermore, the impact pressure of the micro-jet on the skin surface may enhance SC permeability by disrupting SC lipid bilayers (Lee et al. 1998). A micro-jet possessing a radius about one-tenth of the maximum bubble diameter impacts the SC surface without penetrating into it. The impact pressure of the micro-jet on the skin surface may enhance SC permeability by disrupting SC lipid bilayers (Lee et al. 1998). When combined, these factors such as shock waves and micro-jet lead to the disordering of the lipid bilayers and formation of aqueous channels in the skin through which drugs can permeate (Bommannan et al. 1992a).
2.3 Penetration Pathways Induced by Sonophoresis
Cavitation nuclei and air pockets can be formed in the intracellular and/or intercellular structures upon application of ultrasound. In addition, bubbles can be formed on the skin and in the coupling medium on the skin surface. All of these bubbles can be a source of the local inertial and stable cavitation under an ultrasonic field.
2.3.1 Pathways Through Hair Follicles
In addition to the transcellular and intercellular pathways, hair follicle brought attention in TDD as a possible pathway. Although the area occupied by hair follicles is only 0.1 % or less of the total skin surface, the hair follicles appear to play a critical role in passive drug diffusion (Scheuplein et al. 1969; Scheuplein 1967). However, Sarheed and Frum reported that when the hydrocortisone was passively absorbed into the skin, 46 % of absorption involved the drug penetrating into the follicles; however, as the duration of sonication increased, the follicular contribution fell to zero even though total transepidermal flux dramatically increased (Sarheed and Frum 2012). Hence, hair follicles may not be the main pathway in sonophoresis.
2.3.2 Penetration Pathways Through the Stratum Corneum
If we rule out hair follicles as a penetration pathway, there are two other possible pathways: the intercellular route and the transcellular route (see Fig. 2.3). Hydrophilic substances can easily diffuse into the corneocytes and permeate the skin through the transcellular route; however, SC lipid bilayers act as the main barrier for the permeation of these substances (Mitragotri et al. 1995b; Boucaud et al. 2001; Smith 2007; Tezel et al. 2002b; Crum 1984; Tezel et al. 2003). Alvarez-Román et al. have shown that sonophoresis leads to lipid extraction in the SC, i.e., they found that approximately 30 % of lipid can be removed during sonophoresis (Alvarez-Román et al. 2003). Under this assumption, a number of aqueous porous membrane models were suggested and modified to explain the intercellular pathway (Edwards and Langer 1994; Mitragotri 2001; Tezel et al. 2003; Mitragotri and Kost 2004; Paliwal et al. 2006; Polat et al. 2011a, b). Based on these models, Tezel et al. (2003) implied that the increase of porosity of the SC, leading to an enhanced skin permeability, is also responsible for the penetration enhancement induced by sonophoresis. Lavon et al. suggested that the growth of bubble due to rectified diffusion can be the reason of increased porosity (Lavon et al. 2007). Several researchers also paid attention to the heterogeneous nature of the skin where sonophoresis was applied uniformly (Kushner et al. 2008a; Polat et al. 2011a). The spots which are called localized transport regions (LTRs) can be observed on the completion of sonophoresis, and LTRs are believed to be the localized channel opening of a tortuous intercellular route.
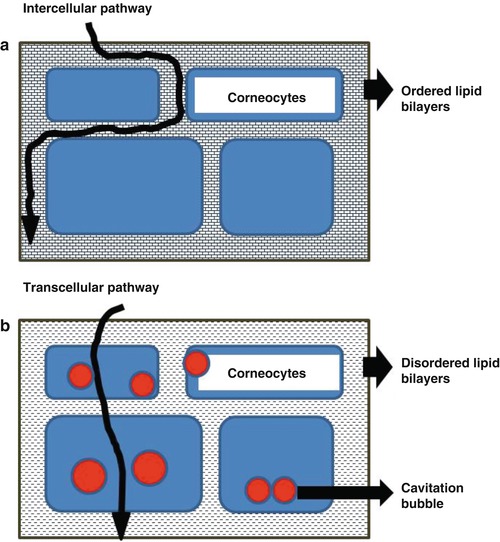
Fig. 2.3
Schematic illustrating representation of the transport penetration pathways during (a) passive transport and (b) low-frequency sonophoresis (The figure is reproduced with permission from Mitragotri et al. 1996)
In summary, some researchers claim that stable cavitation inside the epidermis may cause the growth of lacuna and create larger space to be transport channels (Paliwal et al. 2006). Other researchers believe that multiple events of inertial cavitation on the surface of the skin and inside the epidermis lead to the formation of shock waves, which then microscopically disrupt the lipid bilayers and eventually create pathways through the tortuous intercellular lipid layers with causing significant structural changes in the epidermis.
2.3.3 Transcellular Pathways
Micro-jet can be formed on the epidermis surface. Micro-jets can be strong enough to create pits on aluminum surface and biological tissue. Lee et al. have observed 1–2 μm size pits on the epidermis on the completion of sonophoresis lasting for 5 min (Lee et al. 2010). Based on the visualized evidence and the micro-jet idea, a direct channel formation through transcellular region can be hypothesized. Cavitation on the skin surface is critical in this hypothesis, and the other research results support that transient cavitation outside the skin is the key mechanism responsible for LFS-induced skin permeabilization (Tang et al. 2002; Wolloch and Kost 2010) and the observation of LTRs can be also coped with this hypothesis as well.
Based on the evidence, both intercellular pathway and transcellular pathway appear to be plausible, but the major transport pathway is through the intercellular lipid domains. Further research will be required to clarify the main penetration pathways during sonophoresis-induced TDD.
2.4 Synergistic Effect of Low-Frequency Sonophoresis and Other Enhancers for Transdermal Drug Delivery
Previous studies have demonstrated that sonophoresis may act synergistically with other penetration enhancement methods on transdermal drug delivery (Mitragotri and Kost 2004). Low-frequency sonophoresis acts synergistically with various chemical penetration enhancers. Mitragotri et al. (Mitragotri et al. 2000a) reported that sodium lauryl sulfate enhanced skin permeability to mannitol synergistically in combination with ultrasound. Johnson et al. (Johnson et al. 1996) reported that combined application of linoleic acid and ethanol with ultrasound increased corticosteroid flux by up to 13,000-fold compared with passive flux, which was higher than that induced by each treatment alone. The proposed mechanism for these synergistic effects of ultrasound and chemical penetration enhancers on TDD is that the cavitation produced by ultrasound may induce mixing and dispersion of the chemical enhancer with SC lipids (Johnson et al. 1996). In addition, ultrasound combined with iontophoresis has been shown to have synergistic effect on enhancing heparin flux though the skin (Le et al. 2000). The possible mechanism for the synergistic effect of ultrasound and iontophoresis for transdermal drug delivery includes the decrease of skin’s impedance and size selectivity of the skin due to ultrasound-induced structural changes in the skin (Le et al. 2000). Ultrasound has been demonstrated to have synergistic effect for transdermal drug delivery when combined with electroporation. Kost et al. (1996) has reported that simultaneous application of ultrasound and electroporation enhanced transdermal delivery of two molecules, calcein and sulforhodamine. The possible mechanism for this synergistic effect of ultrasound and electroporation on transdermal drug delivery might be reduced skin impedance, enhanced convection, and reduced size selectivity of the skin (Le et al. 2000; Kost et al. 1996).
2.5 Factors Affecting Drug Delivery by Low-Frequency Sonophoresis
As indicated in the section regarding to the mechanism, cavitation appears to be the main mechanism in sonophoresis. Accordingly, the factors facilitating cavitation will be the key factors affecting drug delivery. The first factor is the ratio of frequency and peak rare-fractional pressure (also called peak-negative pressure) as explained in mechanical index (MI). Since low-frequency and high rare-fractional pressure increase MI, the inertial cavitation is more likely to occur at low-frequency sonophoresis. When the frequency is low enough, the given acoustic field can be assumed to be a quasi-static field. If small bubbles can rapidly grow and collapse with exposure to quasi-static rare-fractional pressure, these bubble activities can be related to inertia cavitation or asymmetric bubble collapse. Low-frequency sonophoresis has thus been the topic of extensive research over the last 20 years. The effects of low-frequency sonophoresis have been studied by Mitragotri et al. (Mitragotri et al. 1995a, 1996) to enhance the transport of various low-molecular weight drugs (including aldosterone, corticosterone, estradiol, histamine, mannitol, salicylic acid, and sucrose) as well as high-molecular weight drugs (such as heparin and insulin). They also found that the enhancement ratio induced by low-frequency sonophoresis (20 kHz) is 1000-fold higher than that induced by therapeutic sonophoresis (1–3 MHz). The results of several studies suggest that the greater efficiency of low-frequency sonophoresis compared with high-frequency sonophoresis originates from the increased incidence of cavitation events (Mitragotri et al. 1996; Tezel et al. 2001). The distance between the surface of transducer and the skin surface was also mentioned as a factor influencing the TDD by ultrasound in some articles (Terahara et al. 2002). However, the peak-negative pressure decreases as the distance increases, and hence the possibility of cavitation decreases accordingly. More importantly, the occurring level of cavitation could be the second factor influencing the efficacy of the TDD by ultrasound, since cavitation bubbles nucleating and collapsing on the SC surface are likely to make a significant contribution to permeabilization of the SC due to their proximity (Tang et al. 2002; Tezel et al. 2003). Tezel et al. (2003) suggested that only cavitation which occurs within 50 μm from the skin surface could effectively increase skin permeability. The third and the fourth factor affecting the efficacy of the TDD by ultrasound are the viscosity and the composition of the gas and liquid phases of drug where permeants are dissolved. In viscous medium, higher pressure is required to cause inertial cavitation since the viscous medium absolves mechanical energy by damping (Tang et al. 2002; Popinet and Zaleski 2002). On the other hand, solute highly saturated with gas can experience cavitation with small ultrasonic perturbation since small gas bubbles can act as cavitation nuclei (Ueda et al. 2009). In recent studies, Park et al. utilized even the ultrasound contrast agents, which are engineered microbubbles of a certain size distribution, to increase cavitation induction (Park et al. 2010; Polat et al. 2011b). Further studies will be needed to draw a definite conclusion regarding this factor (Cagnie et al. 2003; Sarheed and Abdul Rasool 2011; Herwadkar et al. 2012).
2.6 Therapeutic Application of Sonophoresis
Various applications of sonophoresis in TDD are summarized in Table 2.1.
Table 2.1
Studies using sonophoresis in TDD
Compound | MW [Dalton] | Skin tissue | Ultrasound parameter | Reference | |||
|---|---|---|---|---|---|---|---|
Frequency | Intensity | Sonication time | Duty | ||||
Aldosterone | 360 | Human (in vitro) | 20 kHz | 125 mW/cm2 | 10 % | Mitragotri et al. (1996) | |
Ascorbic acid | 176 | Pig ear (in vitro) | 1 MHz | 2.3, 3.2 W/cm2 | 1, 10, 20 min | CW mode | Ngamratanapaiboon et al. (2012) |
Butanol | 74 | Human (in vitro) | 20 kHz | 125mW/cm2 | 10 % | Mitragotri et al. (1996) | |
Caffeine | 194 | Pig (in vitro) | 3 MHz | 0.2 W/cm2 | 240 min | CW mode | Pires-de-Campos et al. (2007) |
Caffeine | 194 | Human (in vitro), Rat (in vitro) | 20 kHz | 2.5 W/cm2 | 10 min, 1 h | CW mode 10 % | Boucaud et al. (2001) |
Caffeine | 194 | Pig (in vitro) | 20 kHz | 0.37–3.7 W/cm2 | 5–1200 s | 10, 33, 100 % | Sarheed and Abdul Rasool (2011) |
Calcium | 40 | Rat (in vivo) | 20 kHz | 1 W/cm2 | Less than 5 min | 50 % | Mitragotri and Kost (2000) |
Corticosterone | 346 | Human (in vitro) | 20 kHz | 125 mW/cm2 | 10 % | Mitragotri et al. (1996) | |
Dexamethasone | 392 | Human (in vivo) | 1, 3 MHz | 1 W/cm2 | 10 min | CW mode | Darrow et al. (1999) |
Diclofenac | 296 | Human (in vivo) | 1 MHz | 0.5 W/cm2 | 5 min | Rosim et al. (2005) | |
Estradiol | 272 | Human (in vitro) | 20 kHz | 125mv/cm2 | 10 % | Mitragotri et al. (1996) | |
Fentanyl | 336 | Human (in vitro), Rat (in vitro) | 20 kHz | 2.5 W/cm2 | 10 min, 1 h | CW mode 10 % | Boucaud et al. (2001) |
FITC-dextran | 4000, 20,000, 150,000 | Rat (in vivo) | 1.12, 2.47 MHz | 330 mW/cm2 | 30 min | 1 % | Park et al. (2012) |
Glycerol | 92 | Pig (in vitro) | 1.1 MHz | 600kPa | 60 min | 10 % | Park et al. (2010) |
Heparin | Average MW of 18,000 | Pig (in vitro) | 20 kHz | 7 W/cm2 | 10 min | 50 % | Mitragotri and Kost (2001) |
Histamine | 184 | Human (in vivo) | 36 kHz | 2.72, 3.50 W/cm2 | 5 min | 28.6, 37.5 % | Maruani et al. (2010) |
Hyaluronan | 1000 | Rabbit (in vivo) | 1 MHz | 400 mW/cm2 | 10 min | CW mode | Park et al. (2005) |
Hydrocortisone | 362 | Human (in vitro) | 20 kHz | 3.7 W/cm2 | 30, 45 s | 10 % | Sarheed and Frum (2012) |
Insulin | 5807 | Rabbit (in vivo) | 105 kHz | 5kPa | 90 min | 50 % | Tachibana (1992) |
Insulin | 5807 | Human (in vitro) | 20 kHz | 12.5 – 225 mW/cm2 | 4 h | 10 % | Mitragotri et al. (1995b) |
Insulin | 5807 | Human (in vitro) | 20 kHz | 173.7 ± 1.2 mW/cm2 | 1 h | 20 % | Smith et al. (2003) |
Insulin | 5807 | Rabbit (in vivo) | 20 kHz | 100 mW/cm2 | 20 % | Lee et al. (2005) | |
Insulin | 5807 | Pig (in vivo) | 20 kHz | 100 mW/cm2 | 60 min | 20 % | Park et al. (2007) |
Insulin
Related posts: Microporation in Penetration Enhancement Microporation in Penetration Enhancement
 Combined Use of Ultrasound and Other Physical Methods of Skin Penetration Enhancement Combined Use of Ultrasound and Other Physical Methods of Skin Penetration Enhancement
 Skin Vaccination Methods: Gene Gun, Jet Injector, Tattoo Vaccine, and Microneedle Skin Vaccination Methods: Gene Gun, Jet Injector, Tattoo Vaccine, and Microneedle
 Electroporation for Dermal and Transdermal Drug Delivery Electroporation for Dermal and Transdermal Drug Delivery
 Therapeutic Applications of Electroporation Therapeutic Applications of Electroporation
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

| |||||||