20 The masseters and their treatment with botulinum toxin
Summary and Key Features
• The masseter muscle may become hypertrophied distorting the mandibular angle
• Masseteric hypertrophy may be a cause of bruxism and facial pain syndromes
• Botulinum toxin may be used to treat both medical pain syndromes and to change facial shape by changing the mandibular angle
• Botulinum toxin may replace surgical and orthodontic techniques in selected patients in both medical and aesthetic indications
• Botulinum toxin may allow us to beautify patients by altering the lower facial width and converting the face to a more youthful triangular or heart-shaped face
History
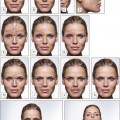
Evidence has begun to accumulate that the masseteric hypertrophy has other effects besides the bulk it directly confers because of the muscle volume. In line with theories of bone deposition and development, Wu found in 2010 that this muscle development may have effects on the underlying bone growth and volume. Bone growth and volume are under the influence and related to the activity of the muscles attached to the bone. A bone responds to the activity and strength of the muscles attached to it by thickening and the corollary is that bone will decrease when the muscular force acting on the bone is decreased, as reported by Tsai et al. Molina et al found that the masseter neuromuscular end plates are developed by 12 weeks’ fetal gestation. By restraining mouth opening, Habib and co-workers showed by the use of suturing that restricted fetal temporomandibular joint movement influences the process of endochondral bone formation of condylar cartilage. These effects on bone may explain the trimming effect that botulinum toxin has on the facial shape may be above and beyond the effects of what would be expected by a decrease in muscle bulk alone (Fig. 20.1). However, not all authors (e.g. Chang et al) believe that bony resorption occurs after botulinum toxin injection.


Anatomy
Masseter muscle
1. The superficial part arises from the zygomatic process of the maxilla and from the anterior two-thirds of the lower border of the zygomatic arch
2. The middle part originates from the deep surface of the anterior two-thirds of the zygomatic arch and from the lower border of the posterior one-third of the arch
3. The deep part arises from the deep surface of the zygomatic arch.
Surface anatomy of the masseter muscle
The muscle is easily outlined, with the superior border represented by the zygomatic arch and the inferior border being the inferior border of the mandible, The posterior border is the posterior border of the mandible, and the anterior border is easily seen in those with hypertrophy by asking the patient to clench their teeth. Anteriorly, along the jawline the masseter muscle will give way to a gap where often the arterial pulsation of the facial artery may be felt, and superior to this the hardness of the contracting masseter muscle may be contrasted with the softer connective tissue of the face anterior to the contracting muscle (Fig. 20.2).



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


