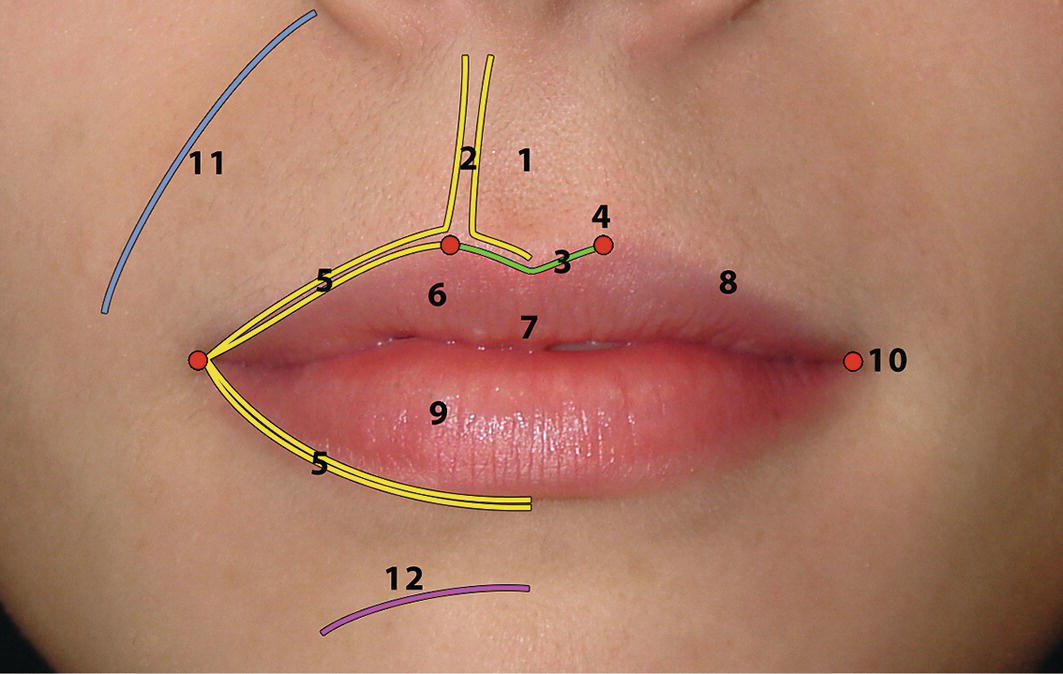
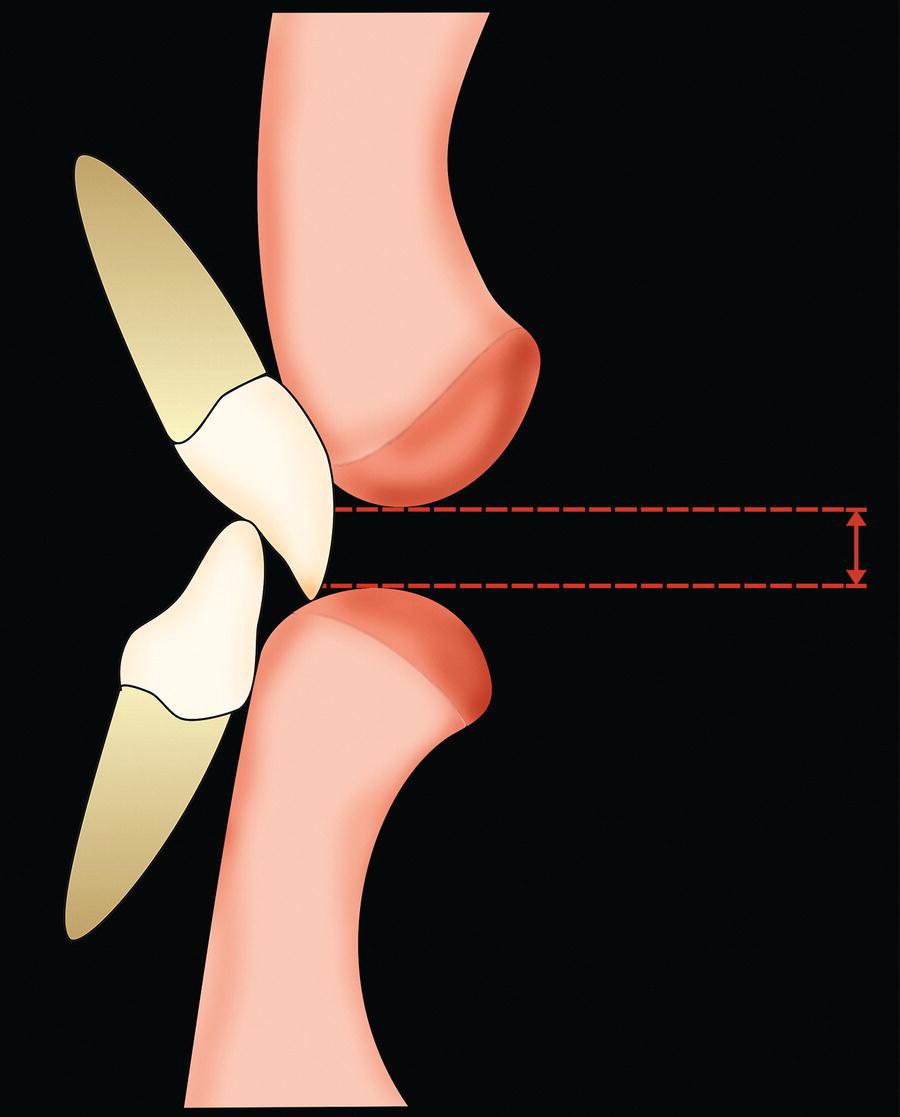
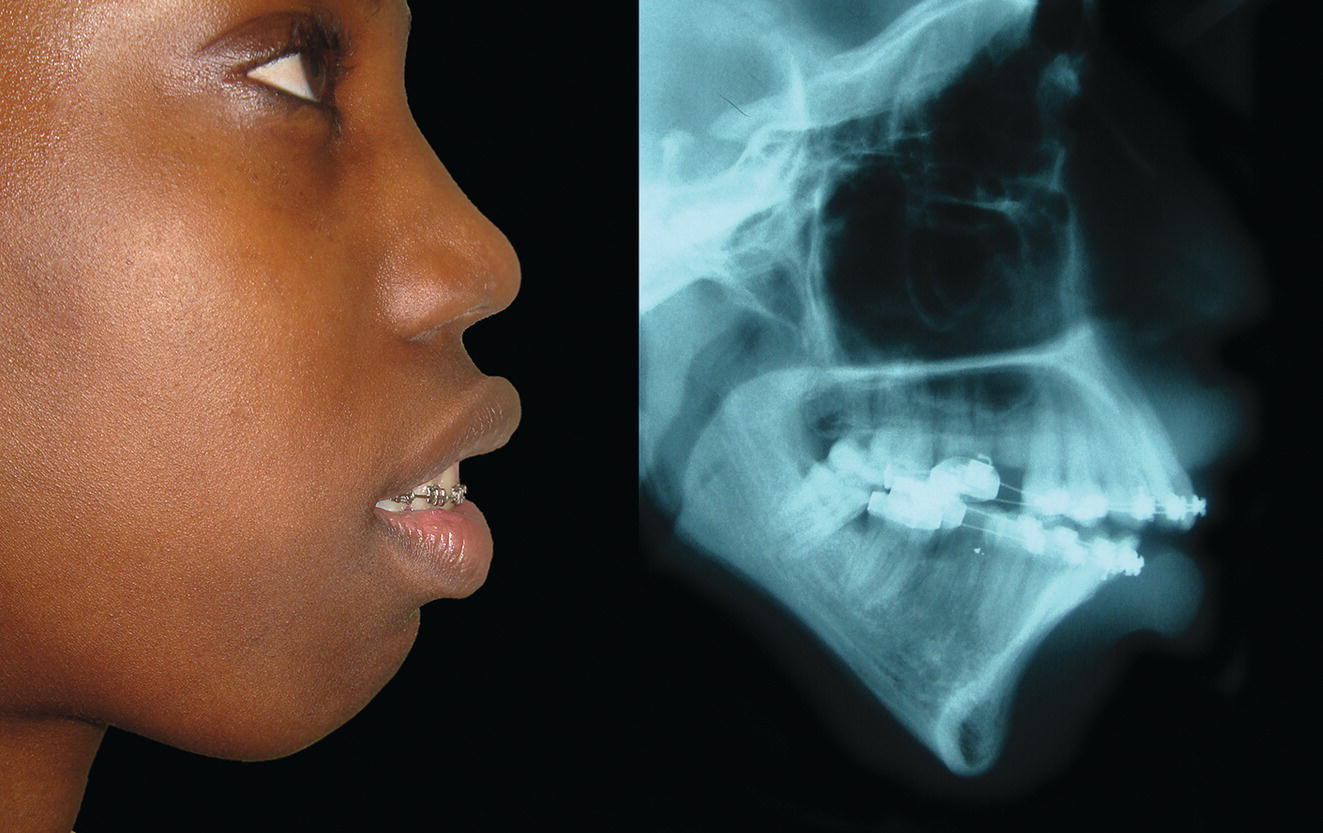
The lips form a transition zone between the facial skin and the oral mucosa and are a significant aesthetic feature of the face (Figure 17.1). They serve important functional roles in phonation and the formation of an anterior oral seal in swallowing. The vermilion of the lips is highly sensitive to light touch sensation and is represented by a large area in the sensory cortex. It is the main exploratory area in babies, before they learn to use their hands for stereognosis. The lips are perhaps the most movable expressive aesthetic unit of the face. Leonardo da Vinci described the importance of the ‘strongly movable section of the face around the mouth and chin in determining facial expression’, which emphasizes the importance of observing the face in animation as well as in the static state.2 Figure 17.1 The lips are a significant aesthetic unit of the face. (Detail, Ginevra de’ Benci, c. 1476–8, Leonardo da Vinci, National Gallery of Art, Washington.) The upper lip forms from fusion of the bilateral maxillary processes with the midline medial nasal process. The characteristic morphology of the philtral ridges and Cupid’s bow of the upper lip are a reflection of this developmental process; a cleft lip is a manifestation of this process going wrong (Figure 17.2). The lower lip forms from the fusion of the two mandibular processes, resulting in a simpler and less defined structure. The lips form an aesthetic unit of the face and are anatomically and aesthetically comprised of a number of subunits (Figure 17.3). Figure 17.2 Repaired right‐sided cleft lip. Figure 17.3 Lip anatomy and terminology: Figure 17.4 Changes in lip morphology with ageing. Lip morphology will tend to change with advancing age (Figure 17.4). However, the ageing process is exacerbated by extrinsic factors, such as excessive sun exposure and smoking. Lip size tends to increase until puberty, due to muscular and glandular hypertrophy, following which it begins to decrease due to changes in the skin and the supporting tissues, including the muscle, adipose tissue and the maxillary and mandibular dentoalveolus. The following changes tend to occur with the ageing process: Labial, labio – (Greek labium: lip). Oral, oro – (Latin oris: mouth). Lip protrusion: Refers to an excessively anterior position of the upper or lower lips relative to the facial profile, particularly the nose and chin. Protrusion of both lips is referred to as bilabial protrusion. Lip retrusion: Refers to an excessively posterior position of the upper or lower lips relative to the facial profile, particularly the nose and chin. Retrusion of both lips is referred to as bilabial retrusion. Lip procumbence: (Latin procumbere: ‘to fall forwards’) a term used to describe a lower lip that is literally ‘falling forwards’. Procumbence is a description of lip morphology rather than position. Individuals with mandibular deficiency and reduced lower anterior face height (LAFH) will often have a lower lip that is both retrusive and procumbent. Systematic clinical evaluation of the lips requires analysis of a number of parameters, which may be conveniently remembered with the acronym LAMPP: lip lines, activity (function), morphology (form), posture and prominence. Lip lines are defined as the vertical position of the upper and lower lips in relation to the anterior dentition. The ‘ideal’ dentolabial relationship results when the upper lip covers approximately the upper two‐thirds of the maxillary incisor crowns at rest, with 2–5 mm maxillary incisor exposure. The interlabial separation is no more than 2–3 mm (Figure 17.5). The upper and lower lips may be brought into contact with little or no circumoral contraction, with the lower lip covering the incisal third of the maxillary central incisors. Figure 17.5 Resting lip lines: The interlabial separation is no more than 2–3 mm in repose. Figure 17.6 High upper lip line. Figure 17.7 Low upper lip line: The maxillary incisor display may be non‐existent at rest and in extreme cases, in speech and in smiling. Figure 17.8 High lower lip line: The lower lip often rests high on the labial (facial) surface of the maxillary central incisors in Class II division 2 malocclusion, sometimes covering the entire labial surface of the maxillary incisors; pressure from the lower lip is sufficient to retrocline the maxillary central incisors as they erupt. Clinical evaluation of lip lines is discussed further in Chapter 23. This refers to the muscular tone of the lips, related to the production of normal muscular contraction and function. The terms hypertonic or hypertonicity refer to a state of abnormally high muscle tone, sometimes described as hyperactivity or overactivity, which is common in Class II division 2 malocclusion, and tends to retrocline the incisor teeth; in Class II division 1 malocclusion, a hypertonic lower lip may retrocline the mandibular incisor teeth (Figure 17.9). The term strap‐like lower lip is sometimes used to describe such overactivity. Figure 17.9 Hypertonicity of the lower lip. The terms hypotonic or hypotonicity refer to a state of abnormally low muscle tone, sometimes described as underactivity. Hypotonicity of the upper lip is common in patients with increased lower face height or severe skeletal Class II jaw relationship combined with lip incompetence (Figure 17.10). The lack of function and hypotonicity is due to the anterior oral seal being formed by the tongue and lower lip, without the contraction of the upper lip. Correction of the underlying deformity allows normal lip function and often results in the upper lip developing normal tonicity. In bimaxillary protrusion and/or proclination the lips tend to be soft and rather limp, sometimes described as flaccid (Figure 17.11). As such they offer very little resistance to the labial surface of the teeth and may be involved in the aetiology of the proclination due to the greater tongue pressure on the lingual surface of the incisor teeth. Lip height, also referred to as lip length, should be evaluated in terms of absolute linear measurements compared to population norms (Table 17.1) and the proportional relationship between the upper to the lower lips. Figure 17.10 Hypotonicity of the upper lip. Figure 17.11 Flaccid lips. Table 17.1 Upper lip height Mean adult population norms, measured from subnasale to stomion superius, in mm. Figure 17.12 In Class II division 1 malocclusion the lower lip will form a seal behind the maxillary incisors; this leads to adaptive patterns of lip and tongue activity in order to form an anterior oral seal in deglutition.
Chapter 17
The Lips
Introduction
Anatomy
Embryology
Anatomy


Ageing
Terminology
Clinical evaluation
Lip lines



Lip activity (function)
Lip tonicity

Dynamic lip evaluation
Lip morphology (form)
Lip height

Study
Caucasian
Chinese*
Black (African American)*
Male
Female
Male
Female
Male
Female
Burstone (1967)3
23.8 ± 1.5 (range: 21.5–26.0)
20.1 ± 1.9 (range: 17.0–23.0)
Farkas et al.4,5 (1984; 1994*)
21.8 ± 2.2
19.6 ± 2.4
23.5 ± 2.2
21.6 ± 2.1
26.1 ± 2.5
24.5 ± 3.0
Peck et al.6 (1992)
23.4 ± 2.5
21.2 ± 2.4
Bhatia and Leighton7 (1993)
21.8 ± 1.7
20.9 ± 2.5

Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


