Fig. 23.1
Clinical picture of vitiligo in a Filipino (a) and histopathology (b) showing absence of melanocytes and melanin in the basal cell layer (arrow) (H & E, × 40)
Fig. 23.2
(a) Melanocytes showing apoptosis (arrow) may be seen in some biopsies with either follicular repigmentation or at the edge of the lesion; (b) A lymphocyte (arrow) is present next to an apoptotic melanocyte (H & E, ×400)
In a recent study done by Wang et al. [11] in 20 patients diagnosed with non-segmental vitiligo, the immunohistochemical marker Melan-A was used to quantify melanocytes in normal-appearing lesional skin, depigmented lesional skin, and the leading edge skin from vitiligo lesions. Abundant expression of Melan-A was observed in pigmented lesional skin, highlighting melanized keratinocytes and melanocytes found at the dermoepidermal junction (DEJ). By comparison, melanocytes were absent, and no positivity was observed in depigmented lesional skin samples. However, staining of the leading edge of depigmented vitiligo skin showed fewer Melan-A-positive cells (Fig. 23.3a), which are apoptotic and show distorted cellular morphology (Fig. 23.3b, c).
Fig. 23.3
Immunohistochemistry of the leading edge of depigmented vitiligo skin shows markedly decreased number of Melan-A-positive melanocytes in the basal cell layer (a) and highlights apoptotic melanocytes showing distorted morphology (arrows, b, c) (Melan-A stain ×400)
The number of epidermal Langerhans cells is greater in the leading edge and lesional skin as compared to non-lesional skin, shown through the use of immunohistochemical markers CD207/Langerin and CD11c. The Langerhans cells reside in the lower half of the epidermis in contrast to non-lesional pigmented skin where they are uniformly distributed in the stratum malphigi. More mature and activated Langerhans cells are found in the leading edge vitiligo skin compared to non-lesional and depigmented lesional skin as demonstrated by the markers HLA-DR+ and DC-LAMP+ [11].
23.3 Dermis
A review of 74 vitiligo specimens revealed (1) perivascular mononuclear inflammatory cell infiltrates in 30 %, (2) sweat gland degeneration in 72 %, (3) sebaceous gland/hair follicle degeneration in 38 %, and (4) nerve degeneration in 78 % [8] (Fig. 23.4a). A mild lymphocytic infiltrate in the upper dermis is a common finding [12] (Fig. 23.4b).
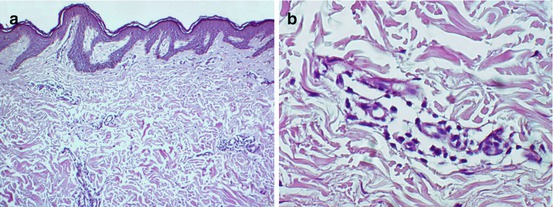
Fig. 23.4
(a) The dermis reveals decreased number of adnexal structures (H & E ×40) and (b) a mild predominantly lymphocytic inflammatory infiltrate (H & E ×400)
By immunohistochemistry, the pan T-cell marker CD3+ and the cytotoxic CD8+ cells are observed in depigmented lesional skin, further suggesting T-cell-mediated cytotoxicity as one of the mechanisms for melanocyte killing. Also, majority of T cells are found to be both CD3+ and CD4 + (>60 %) [11]. At the leading edge skin of vitiligo lesions, the CD3+ cells are located in the papillary and upper reticular dermis where they form aggregates and are frequently observed to be hugging the basal cell layer or directly infiltrating the epidermis [11]. These cells correspond to the perivascular and focally lichenoid infiltrate of lymphocytes located close to the epidermis (Fig. 23.5a, b).
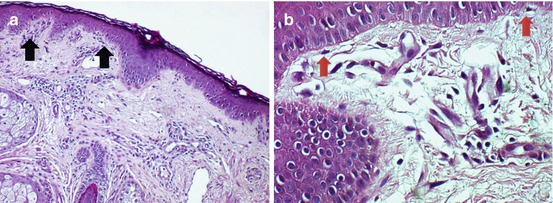
Fig. 23.5
(a) A biopsy on the advancing edge of the lesion shows mononuclear cells in the papillary dermis, either in clumps (black arrows, H & E ×40) or as single cells moving toward the epidermis (red arrows, H & E ×400)
23.4 Special Stains Used in Vitiligo
Useful special stains which can detect both active and dormant melanocytes include HMB45, Mel-5, and NKI/beteb. DOPA detects active melanocytes, and a pan-melanoma cocktail HMB45 + tyrosinase + MART-1 (Melan-A) can maximize yield [13–15].
For research purposes, T-cell CD markers CD3 and CD8 are used to highlight and quantify infiltrating and dermal lymphocytes. CD 207/Langerin, integrin CD11c, HLA-DR, DC-LAMP, and CD83 are additional immunohistochemical stains used to quantify and detect the activity of Langerhans and dermal dendritic cells.
23.5 Differential Diagnosis
23.5.1 Idiopathic Guttate Hypomelanosis (IGH)
IGH is characterized by 2–5 mm hypopigmented or porcelain-white macules usually seen on sun-exposed extremities of the elderly (Fig. 23.6a). Histopathologically, IGH is characterized by hyperkeratosis of the stratum corneum, atrophic epidermis with flattened rete ridges, decreased melanin content, and reduced melanocytes in the basal layer (Fig. 23.6b). In a study by Kim et al. [16] comparing lesional and normal skin, hyperkeratosis was a common feature in patients with IGH, but atrophic epidermis and flattened rete ridges were not. There was also a significantly decreased amount of melanin pigment and detectable melanocytes in the epidermal layers of IGH skin compared to normal skin. The decrease in pigmentation in IGH therefore could be due to decreased number and dysfunction of degenerative melanocytes in addition to a decreased number of melanosomes in some melanocytes.
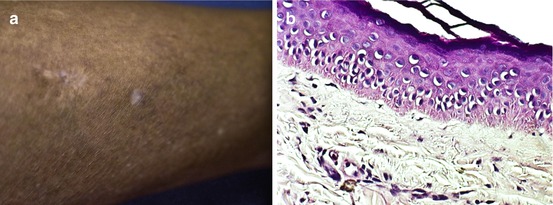
Fig. 23.6
(a) Clinical picture of idiopathic guttate hypomelanosis in brown skin and (b) histopathological findings of flattened rete ridges and markedly decreased number of melanocytes and melanin in the basal cell layer (H & E ×100)
IGH is thus characterized histopathologically by hyperkeratosis, decreased melanin, and melanocytes, in contrast to vitiligo where a complete loss of melanin pigment and absence of melanocytes are seen [9].
23.5.2 Pityriasis Alba (PA)
Pityriasis alba (PA) is characterized by variably hypopigmented slightly scaling patches seen on the face, neck, and shoulders of patients with or without atopic dermatitis (Fig. 23.7a). According to In et al. [17], biopsy specimens of patients assessed with PA revealed spongiosis with exocytosis, hyperkeratosis, and acanthosis in the epidermis; dermal perivascular lymphocytic infiltrates were seen, but not common. The main findings of PA are in the pilar apparatus and include follicular plugging, follicular spongiosis, and atrophic sebaceous glands. There were no significant differences in the number of melanocytes between lesional and normal skin, which both show a normal number of melanocytes in the basal cell layer (Fig. 23.7b). Electron microscopy also revealed degenerative changes in some melanocytes and a reduced number of melanosomes in the keratinocytes from lesional skin.