CHAPTER 11 The “High SMAS” facelift technique
History
The High SMAS technique was developed in the 1980s as a modification of the procedure described by Tord Skoog in 1974.1 Anatomic studies2,3 have documented the benefit of leaving the skin and subcutaneous mass attached to the SMAS in facial rejuvenation.
The initial challenge was to do so, yet still mobilize the cheek mass adequately. The second goal in designing this procedure was to lift the entire malar and mandibular subcutaneous cheek mass, as a single unit suspended by the SMAS.4 No portion of this repositioning technique was to place the skin on any form of greater than normal tension.
Physical evaluation
• Assess the overall quality and volume of the soft tissues.
• Examine the skeletal proportions of the face (height of the maxilla, bi-zygomatic diameter, chin projection, etc.)
• Evaluate the subcutaneous facial fatty mass particularly looking at variations in volume, shape and position. The malar area descends into the upper buccal region, the anterior cheek descends over the nasolabial fold and the buccal fat accumulates as a “jowl”. The shape turns from an oval shape to a squared appearance. Volume changes affect both the amount of improvement without augmentation as well as the sequence of the operation.
• Note whether or not there is shelving of the orbicularis over a prominent malar membrane attachment (malar crescent).
• Assess the depth and prominence of the nasolabial fold as an index of cheek descent.
• Analyze the contour of the fatty cheek mass at the mandibular border by looking for jowls. If present, manually reposition the cheek with the patient sitting and feel the thickness of the jowl fat. Here the prominence of the mandibulocutaneous ligament is assessed.
• Evaluate the resting dermal tension to measure the tone of the patient’s skin. Actinic exposure and smoking deteriorates dermal quality at a much more rapid rate manifesting clinically as fine lines in the perioral area for example.
Technical steps
Begin the dissection by elevating the skin flap in the preauricular area about 4 to 5 cm. Elevate only the skin that you anticipate removing. Perform subcutaneous dissection above the zygomatic arch in the lateral orbital area to release the cutaneous attachments of the crow’s feet and to facilitate a smooth redraping of the temporal skin. This maneuver also exposes the superficial side of the upper SMAS that will be divided later (Fig. 11.1).
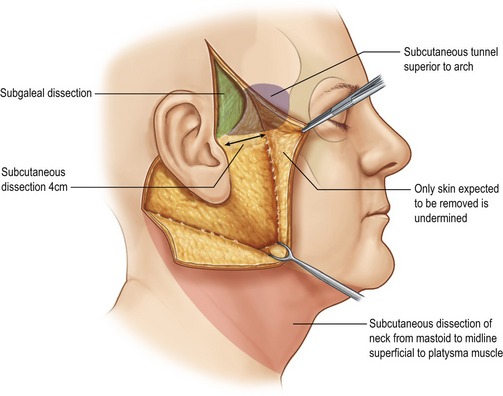
Fig. 11.1 Extent of subcutaneous dissection.
Fritz E. Barton Jr., The ‘high SMAS’ face lift technique. Aesthetic Surgery 2002;22(5):481–486, with permission of Elsevier.
From the mastoid, carry subcutaneous dissection below the mandible to join the anterior neck dissection, if present. In the neck, the skin and platysma are managed as separate layers because more skin than platysmal advancement is desired. A separate submental approach is added when defatting or when midline platysmal plication is indicated (Fig. 11.2).
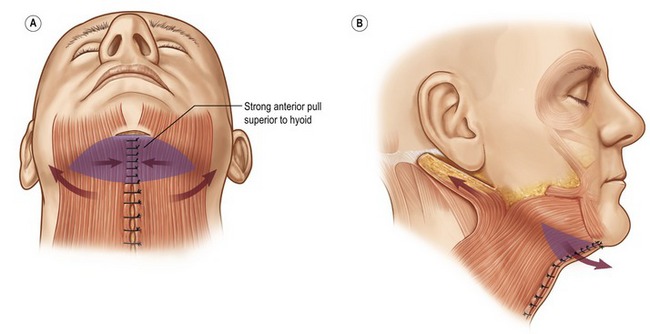
Fig. 11.2 Strong medial tension above the hyoid; lax below the hyoid.
Fritz E. Barton Jr., The ‘high SMAS’ face lift technique, Aesthetic Surgery 2002;22(5):481–486, with permission of Elsevier.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


