Tip suspensory mechanisms have been studied in the past, with theories proposed by Pitanguy, Tardy, Saban, Palhazy, and others, to explain the supporting structures maintaining the nasal tip position. This study introduces the “Fusion Sling” concept, an anatomic interpretation that redefines the understanding of nasal tip stability. The Fusion Sling is a connective tissue structure extending through the pyriform aperture, the cephalic border of the lower lateral cartilages and the medial cruras footplates. It forms a complex network that supports the nasal tip’s position and projection. This study aims to stablish the anatomic and histologic basis for the Fusion Sling.
Key points
- •
“Pitanguy’s ligament” description may be a surgical artifact—the Pitanguy’s flap.
- •
The central and lateral olfactory processes merge to create the Fusion Sling.
- •
The embryologic Fusion Sling of the nose creates different compartments separated from each other by connective tissues.
- •
The Fusion Sling flap may be used in rhinoplasty reconstructions to achieve better, long-lasting results with reduced need for grafting and, consequently, less use of cartilage.
| 3D | three-dimensional |
| ANS | anterior nasal spine |
| ASA | anterior septal angle |
| H&E | Hematoxylin and Eosin |
| LLC | lower lateral cartilage |
| SEG | septal extension graft |
| SMAS | superficial musculoaponeurotic |
| SOON | superficial orbicularis oris nasalis |
| STE | soft tissue envelope |
| TIG | tongue-in-groove |
| ULC | upper lateral cartilage |
| VVG | Verhoeff-Van Gieson |
Video content accompanies this article at http://www.facialplastic.theclinics.com .
Introduction
Nasal tip’s support mechanisms have been a topic of debate and refinement for several decades. Through the years, there has been a—mostly—general consensus on the supporting mechanisms of the nasal tip. Authors like Janeke and Wright, as well as Tardy and colleagues have described a series of ligaments/connections that have led to the acceptance of the “tripod concept” as an accurate description of how the tip position is maintained. The 5 main structures depicted by these authors were (1) the intrinsic strength of the lower lateral cartilages (LLCs); (2) the scroll ligament; (3) the junction between the footplate of the LLC and the septum; (4) the lateral sesamoid ligament; and (5) the interdomal sling. Tardy and colleagues labeled the 3 first structures as the major tip support, and the latter 2 as minor. Other structures like the dermocartilaginous ligament described by Pitanguy and colleagues have also been implied to influence in tip support.
Several of these “ligaments” have been redefined and/or dismissed in consequent dissections. Daniel and Palhazi did not find any fibrous attachments between the medial crura footplate and the caudal septum nor any lateral sesamoid ligament, arising questions regarding their existence and/or their role in tip support. The scroll and the dermocartilaginous or “Pitanguy” ligaments have also been redefined in recent years. Saban and colleagues , described the nasal superficial musculoaponeurotic system (SMAS) as a unique continuous layer consisting of the procerus, transverse nasalis, and compressor minor muscles up to the level of the internal nasal valve. From that point on, it divides into a superficial and deep layer, each with a medial and lateral expansion. The deep medial expansion of the nasal SMAS would correspond with the previously described Pitanguy ligament. The deep lateral expansion consists of vertical fibers with a fatty component that go from the skin to the internal nasal valve, at the level of the scroll ligament. Therefore, a new “Scroll Ligament Complex” has been proposed, in which this structure has 2 components: a horizontal one (as described in earlier dissections) and a vertical component (as recently described). ,
After the anatomic descriptions of these structures made by Anderson, Janeke and Wright, and Tardy and colleagues, the redefinitions made by Saban and colleagues, the surgical applications recommended by Çakir and colleagues, and the more recent anatomic portrayals illustrated by Daniel and Palhazi, these concepts and support mechanisms have been very well integrated into the general rhinoplasty knowledge.
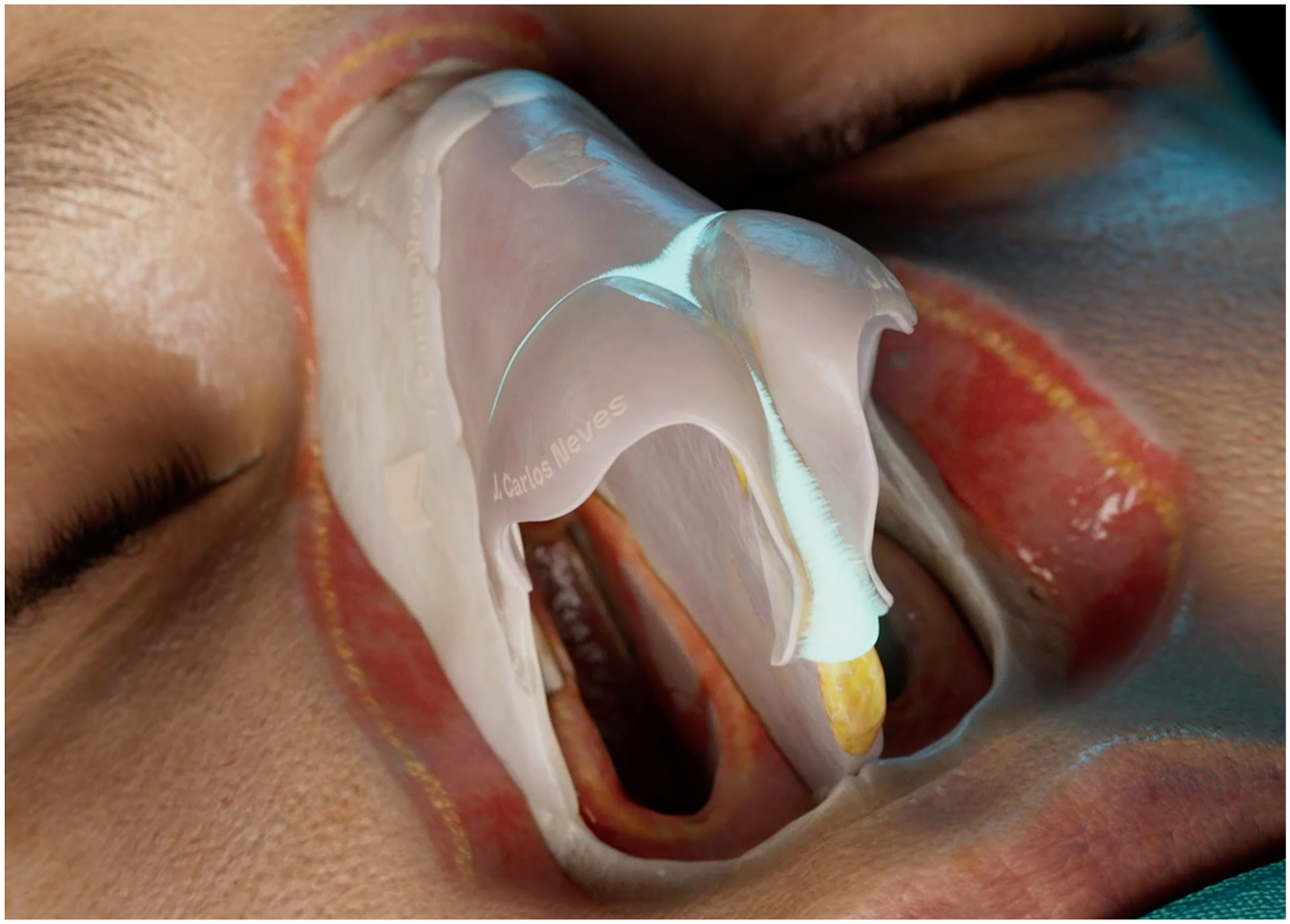
Embryologic studies suggest that nasal anatomy is defined by a complex sequence of invagination and fusion of the “placodes,” or olfactory processes. In the work “ Evo-Devo: The Origin of the Nose, Anterior Skull Base, and Midface ” by Roger Jankowski, an extensive embryologic discussion on how the nose originates is presented. It states that “ phylogenetic considerations suggest that, in human development, fusion of the medial olfactory processes and formation of the intermaxillary process might give rise to the septolateral cartilages, whereas the lateral olfactory processes would give rise to the alar cartilages. (…) the medial olfactory processes of the olfactory pits (moves) from their lateral position to fuse on the midline continues along the midline between the two deepening olfactory sacs with the complete invagination of the medial olfactory process to form the septolateral unit, which as a consequence would bring the lateral olfactory processes to meet caudally of the septolateral cartilage and form the alar cartilages ” ( Fig. 1 ).

Through this merging process, fusion of the lateral olfactory processes toward the midline forms a connective structure that interconnects the cephalic border of the LLCs and functions as a sling. This structure will be referred to in this work as “the Fusion Sling ” ( Fig. 2 ). This sling acts as a continuous suspensory mechanism that stabilizes the nasal tip through a network of connective tissue fibers, extending from the pyriform aperture to the footplates of the medial crura, following the cephalic border of the LLCs. It thereby constitutes an intercompartmental support structure.
At the level of this fusion area, we will focus on describing the connections between these different structures. There are vertical connective tissue densifications between the upper lateral cartilages (ULCs) and the LLC that separate the nasal mid-third from the nasal lower third.
They continue along the cephalic borders of the intermediate and medial crura, extending to the footplates. These densifications are perpendicular to the surface of the LLC and will be referred to as “vertical densifications” in the text. Furthermore, we will describe the horizontal connections of the LLC with neighboring structures. These connections are parallel to the LLCs surface and constitute a continuation of the LLCs and ULCs perichondrium’s—corresponds to the layer 5 of the superficial soft tissue envelope (STE).
We propose that the described Fusion Sling divides the nose in different compartments through its trajectory. At the level of the fusion area, between the upper lateral cartilages (ULC) and the LLC, it separates the mid-third of the nose from the lower third. In the tip-columella complex, it encompasses 3 distinct compartments: the supratip, the intercrural, and the membranous septum compartments.
The purpose of this study is to redefine the concept of nasal tip stability by describing the anatomy of the Fusion Sling and the tip compartments. This article will present an anatomic and histologic analysis of the Fusion Sling, its implications for rhinoplasty, and its role in maintaining nasal tip stability. The findings have significant implications for surgical techniques aimed at preserving and manipulating nasal tip support in rhinoplasty procedures.
Material and methods
Study Design
This study utilized a combination of surgical dissections, cadaveric studies, and histologic analysis to define the anatomy of the nasal tip, focusing on the Fusion Sling and anatomic compartments. Over a period of 4 years, systematic dissections were performed during 537 primary rhinoplasty surgeries. The aim was to map the consistency of the suspensory structures and to identify the compartments created by the Fusion Sling within the nasal tip.
Complementary cadaveric studies were conducted on 23 fresh specimens. Of these, 7 cadaveric noses were injected with colored acrylic ink to delineate specific compartments at the tip midline. Three key areas were selected for ink injection: the space between the medial crura, the supratip region, and the membranous septum. Each of these areas was dissected separately to preserve and define the compartmental boundaries, allowing for precise mapping the nasal tip compartments and the connective denser structures.
Histologic studies were performed in 7 specimens with 2 objectives: (1) to describe and classify the tissues using Hematoxylin and Eosin (H&E) and Verhoeff-Van Gieson (VVG) staining method and (2) to identify and delineate the compartments at the tip region by injecting with Nankin—Chinese ink. Only preliminary results from this histologic study will be evaluated, as we are analyzing more specimens with the ultimate goal of histologically mapping the nasal tip. Even though we present our initial results here, they align with the anatomic dissections previously described.
Cadaveric Injection Studies
Prior to dissection, 3 key areas were injected with different colored inks:
- 1.
Membranous Septum Compartment: The medial crura were pulled forward to expose the membranous septum. The ink was injected through the mucosa, immediately in front of the caudal border of the septum, until tension was felt.
- 2.
Inter-medial Crura Compartment: The ink was injected through the skin at the midpoint of the columella between the 2 medial crural borders until tension was felt.
- 3.
Supratip Compartment: Injection in the midline, immediately above the domal area, in the supratip region. The ink was injected through the skin until tension was felt.
Histologic Studies
Histologic studies were performed using 2 strategies:
- 1.
Coronal and axial cuts of the nasal structure were analyzed with H&E and VVG staining method.
- 2.
With the nose intact, the specimens were injected with Nankin—Chinese ink into the intercrural, membranous septum, and supratip compartments to enhance visualization of the compartment boundaries. The ink was introduced into the compartments following the technique previously described.
Surgical Technique
Surgical dissections followed a standardized protocol to systematically expose and define the layers of the nasal tip:
- 1.
Medial Crura Dissection: Dissection commenced at the caudal border of the medial crura, proceeding in a subareolar plane toward the domal region. The plane was then extended onto the corresponding outer surface of the lateral crura. At the cephalic border of the medial crura, connective tissue densifications linking the medial crura to their contralateral counterparts were identified. This structure, representing an important stabilizing feature, was meticulously preserved, maintaining its attachment to each crura throughout the dissection process.
- 2.
SMAS and Muscular Attachments: The SMAS over the lateral crura and domal areas was identified as a dense fat-connective tissue structure, interspersed with muscle fibers. Key muscles, including the compressor minor and the dilator naris, were marked by increased resistance to dissection, indicating firm attachment points to the perichondrium.
- 3.
Scroll and Supratip Dissection: At the scroll and supratip regions, vertical connective tissue densifications, oriented perpendicularly to the surface of the lateral crus, were observed. These vertical densifications interrupt the continuity between the tip and the mid-third compartments and serve to establish their anatomic boundaries, effectively demarcating these distinct regions. The perichondrium, recognized as the fifth layer of the STE at the cartilage framework, was preferentially preserved throughout the dissection. In the scroll area and in the supratip region, which links the 2 cephalic borders of the lateral crura over the WASA segment (the segment located between the caudal border of the ULC, the W, and the anterior septal angle, ASA) down to the level of the para-septal sesamoid cartilages, a perichondrium-like structure was identified and preserved, when elevating the scroll and tip vertical densification.
- 5.
Compartmental Analysis: The supratip, intercrural, and membranous septum compartments were consistently identified during dissection. Saline injections were utilized intraoperatively to confirm the compartmental integrity, effectively demonstrating the distinct separation of these spaces.
- 6.
After dissecting and elevating the vertical densifications, scroll and supratip, the midline perichondrium-like Fusion Sling was meticulously preserved. At the midline, it was elevated starting at the W region in a caudal progression with the surgeon placed at the head of the patient ( Fig. 3 ). This dissection elevates the Fusion Sling till the level of the footplates, exposing the deeper anatomy, the membranous septum, and the septal caudal border. At this point, a Fusion Sling Flap ( Fig. 4 A ) was produced to be used for tip stabilization.
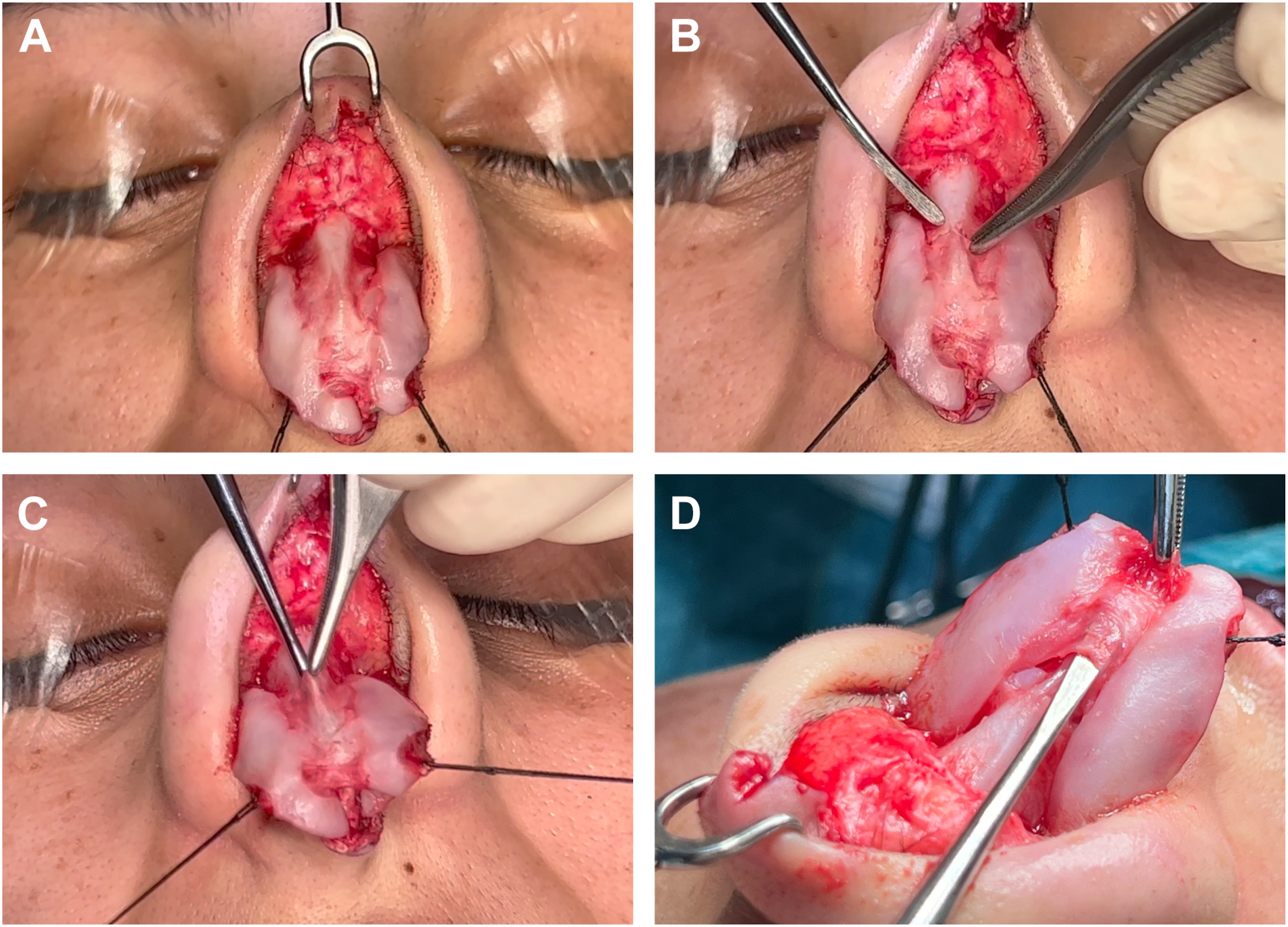
Fig. 3
( A ) The Fusion Sling connecting the ULC and LLC; ( B ) incising the perichondrium at the W region; ( C ) elevating the perichondrium-like Fusion Sling; ( D ) the inter-LLC Fusion Sling.
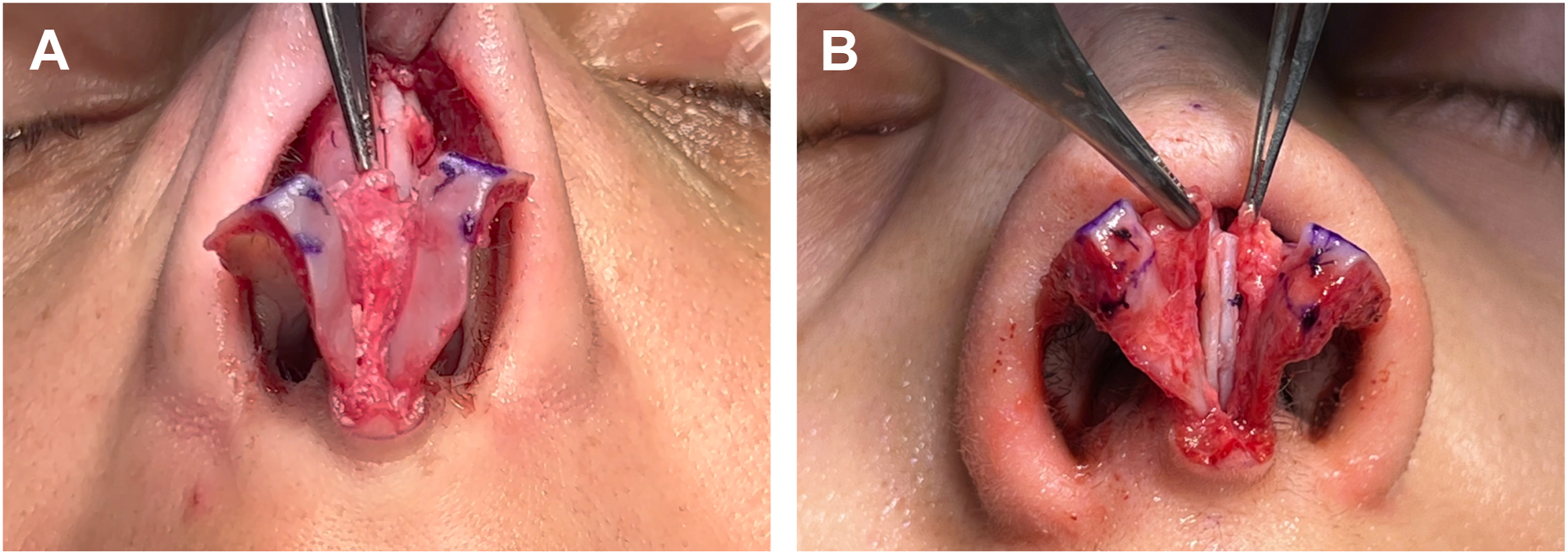
Fig. 4
A ) Fusion Sling flap; ( B ) Hemi-Sling flaps, right and left. The Fusion Sling is split at the midline, maintaining its attachments along the entire length of the cephalic border of the LLC in both hemi-flaps.
- 7.
Intercrural Sling Opening: In cases where transecting the Fusion Sling Flap was necessary, particularly to access the anterior nasal spine (ANS) region, it was carefully performed in the midline. This approach preserved both hemi-Fusion Sling Flaps ( Fig. 4 B) connected to the cephalic border of the correspondent LLCs, thereby maintaining the stabilizing characteristics of the structure. By preserving these connections, after tip reconstruction, the Fusion Sling continued to provide support to the nasal framework.
Results
Cadaveric Findings
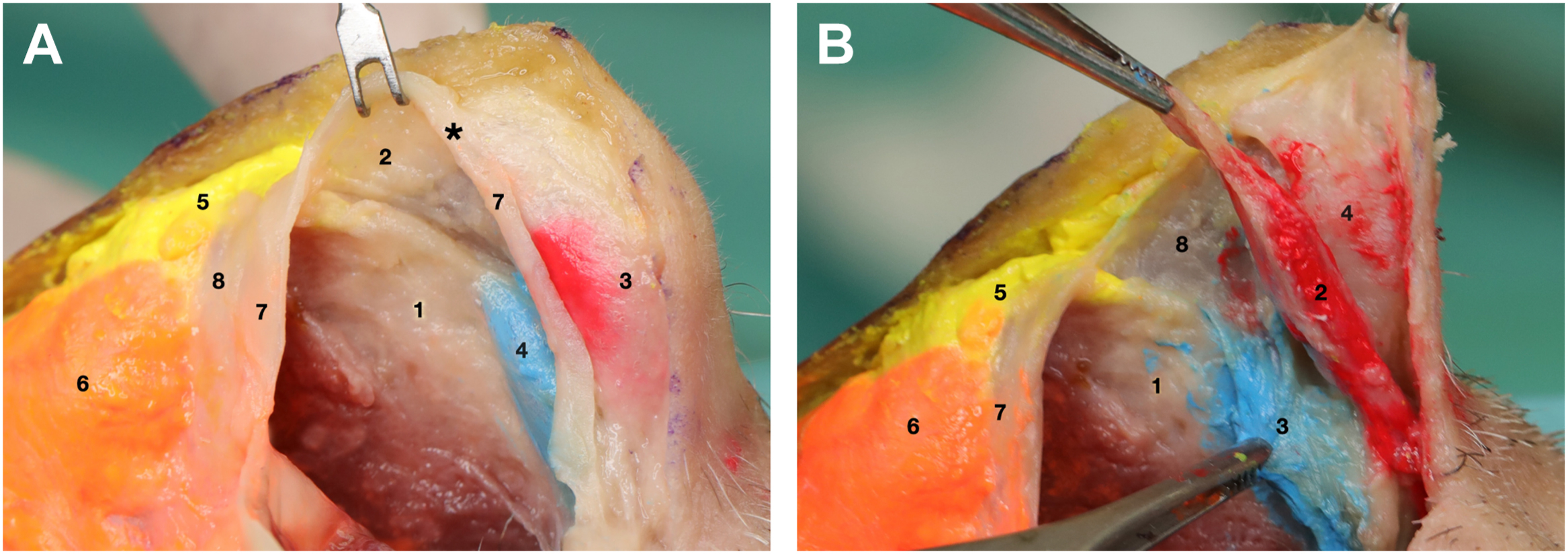
The dissections consistently revealed 3 distinct and independent compartments within the nasal tip complex: the intercrural compartment, the supratip compartment, and the membranous septum compartment. After injecting the acrylic ink, each compartment was delineated by well-defined connective tissue structures, with no intermingling between them ( Fig. 5 ).
Related posts:
 Understanding Dorsal Preservation Rhinoplasty
Understanding Dorsal Preservation Rhinoplasty
 Preservation Rhinoplasty—Outcomes in Dorsal Preservation Rhinoplasty
Preservation Rhinoplasty—Outcomes in Dorsal Preservation Rhinoplasty
 Subdorsal Flaps in Dorsal Preservation
Subdorsal Flaps in Dorsal Preservation
 Expanding Indications to Dorsal Preservation Rhinoplasty
Expanding Indications to Dorsal Preservation Rhinoplasty
 Spare Roof Technique A and B – A Step-by-step Guide to Avoid Suboptimal Outcomes
Spare Roof Technique A and B – A Step-by-step Guide to Avoid Suboptimal Outcomes
 Dorsal Augmentation with Preservation Concepts
Dorsal Augmentation with Preservation Concepts
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


