Antimicrobial peptides are central effector molecules in skin immunology. The functions of antimicrobial peptides in skin diseases include the ability to act as cytokines or growth factors, driving disorders such as psoriasis and rosacea, as well as their action as natural antibiotics to control bacteria that influence diseases such as atopic dermatitis and acne.
Key points
- •
Antimicrobial peptides (AMPs) not only kill bacteria but also control inflammation and other host responses.
- •
The main AMPs that are secreted in skin are cathelicidin and human β-defensins.
- •
Cathelicidin and β-defensins are 2 of many families of antimicrobial peptides in the skin that increase in response to injury.
- •
In psoriatic and rosacea skin, AMPs are overexpressed and promote inflammation. On the other hand, in atopic dermatitis, some AMPs fail to be appropriately induced and enable infection.
- •
Control of the expression and action of AMPs can be of therapeutic benefit for skin diseases.
| AD | Atopic dermatitis |
| AMP | Antimicrobial peptide |
| DAMPs | Danger or Damage-associated molecular patterns |
| FPRL1 | Formyl peptide receptor-like 1 |
| hBD | Human β-defensin |
| HIV | Human immunodeficiency virus |
| IFN | Interferon |
| IL | Interleukin |
| KLK | Kallikrein |
| MCET | Mast cell extracellular trap |
| mDC | Myeloid dendritic cells |
| pDC | Plasmacytoid dendritic cell |
| PSMγ | Phenol-soluble modulin-γ |
| Th cells | T-helper cells |
| TLR | Toll-like receptor |
| TNF | Tumor necrosis factor |
| UV | Ultraviolet |
| VDRE | Vitamin D response element |
Introduction
Skin is the physical and immunologic armor of the body. Both the physical and immune defense system of the skin combine to accomplish functions essential to life, including preventing invasion by pathogenic microbes such as bacteria, fungi, viruses, and parasites, and maintaining homeostasis with commensal microorganisms. Antimicrobial peptides and proteins (AMPs) have an essential role in this immunologic armor and enable epithelial surfaces to cope with many microbial challenges. They are evolutionarily ancient innate immune effectors that are produced by almost all plants and animals. More than 1800 AMPs have been identified and more than 20 AMPs have been found in skin. They typically are small (12–50 amino acids residues), have positive charge and amphipathic structure, features that allow them to interact with negatively charged phospholipid head groups and hydrophobic fatty acid chains of microbial membranes, and kill some organisms by disrupting the microbial membrane and release of cytosol components.
However, AMPs are not only natural antibiotics. Recently, common human skin disorders such as rosacea, psoriasis, and atopic dermatitis (AD) have been linked to an abnormality of AMPs. These skin diseases cannot be attributed only to microorganisms. Contrary to the term antimicrobial, AMPs not only directly kill or inhibit the growth of microorganisms but also modify host inflammatory responses by a variety of mechanisms, including action as chemotactic agents, angiogenic factors, and regulators of cell proliferation. This article summarizes how they participate in human skin diseases and what the knowledge of AMPs will do for clinical dermatology.
Introduction
Skin is the physical and immunologic armor of the body. Both the physical and immune defense system of the skin combine to accomplish functions essential to life, including preventing invasion by pathogenic microbes such as bacteria, fungi, viruses, and parasites, and maintaining homeostasis with commensal microorganisms. Antimicrobial peptides and proteins (AMPs) have an essential role in this immunologic armor and enable epithelial surfaces to cope with many microbial challenges. They are evolutionarily ancient innate immune effectors that are produced by almost all plants and animals. More than 1800 AMPs have been identified and more than 20 AMPs have been found in skin. They typically are small (12–50 amino acids residues), have positive charge and amphipathic structure, features that allow them to interact with negatively charged phospholipid head groups and hydrophobic fatty acid chains of microbial membranes, and kill some organisms by disrupting the microbial membrane and release of cytosol components.
However, AMPs are not only natural antibiotics. Recently, common human skin disorders such as rosacea, psoriasis, and atopic dermatitis (AD) have been linked to an abnormality of AMPs. These skin diseases cannot be attributed only to microorganisms. Contrary to the term antimicrobial, AMPs not only directly kill or inhibit the growth of microorganisms but also modify host inflammatory responses by a variety of mechanisms, including action as chemotactic agents, angiogenic factors, and regulators of cell proliferation. This article summarizes how they participate in human skin diseases and what the knowledge of AMPs will do for clinical dermatology.
Antimicrobial protein function: basic
Key AMPs of the skin’s repertoire are the cathelicidins, the first AMP discovered in mammalian skin and β-defensins. The single cathelicidin gene ( CAMP ) encodes a precursor protein, hCAP18 in humans. This protein can be alternatively cleaved to generate several active AMPs, including the 37-amino-acid peptide LL-37. In contrast to cathelicidin, approximately 90 β-defensin genes have been identified in mice and humans. Both cathelicidins and β-defensins are antimicrobial against a diverse range of skin pathogens, including gram-negative and gram-positive bacteria, fungi, viruses, and parasites. In normal skin, keratinocytes produce various AMPs at lower levels to defend the skin barrier, whereas cathelicidin precursor protein and mature peptide are the most abundantly expressed by resident mast cells. Mast cells normally occupy positions around blood vessels and store large amounts of cathelicidin in preformed granules. This localization places the AMPs derived from mast cells in an ideal position to resist infections after skin injury and inoculation with pathogens. Moreover, AMPs has been detected in mast cell extracellular traps (MCETs). Once inflamed, skin produces cathelicidin through increased expression of CAP18 by keratinocytes, adipocytes, and increased local deposition by recruited neutrophils.
Though many AMPs target essential cell wall or cell membrane structures through enzymatic or nonenzymatic disruption, AMPs can also function as potent immune regulators by signaling through chemokine receptors and by inhibiting or enhancing Toll-like receptor (TLR) signaling. AMPs seem to function not only under stimulus from pathogen-associated molecular patterns but also as triggered by danger-associated or damage-associated molecular patterns, including urea and nucleic acids. This means that AMPs are not only antimicrobial.
The expression, secretion, and activity of most AMPs are tightly controlled. Cathelicidins are synthesized as propeptides. Serine proteases are responsible for the processing of cathelicidins into various sizes. In neutrophils, the propeptide is removed by proteinase 3, whereas processing is carried out by kallikreins (KLKs, also known as stratum corneum tryptic enzyme) in keratinocytes. Interestingly, the antimicrobial activity of cathelicidin peptides differs by their size. Processing mechanisms generate the active forms of AMPs in skin and the mechanism is useful to prevent potential harmful effects of these proteins on mammalian cell membranes. A particularly surprising observation came with the recognition that the human cathelicidin gene is under transcriptional control of a vitamin D response element (VDRE). Following skin injury or infection, 25(OH)D3 is hydroxylated by the enzyme cytochrome p450, 27B1 (CYP27B1) to 1,25(OH) 2 D3, and this is stimulated locally by activation of TLR2 or local cytokines such as tumor necrosis factor (TNF) or type I interferons (IFNs). This local enzymatic event enables rapid induction of CAMP expression through binding of 1,25(OH) 2 D3 to the VDRE. These observations suggest that AMP expression could be influenced by serum vitamin D level, dietary vitamin D, or vitamin D generated by exposure of the skin to sunlight. This implies that the nutritional environment is probably a source of important signals that control AMP expression. Conversely, LL-37 also transactivates epidermal growth factor receptor and downstream signaling in epithelial cells.
Similarly, β-defensins are expressed as propeptides; however, the processing mechanism remains to be established.
Antimicrobial protein function in vivo
AMPs not only provide resistance to infection by killing bacteria but may also determine microbiota composition and limit access of the microbiota to host tissues. Surprisingly, an important component of the surface antimicrobial shield of the skin is produced by the resident microorganisms themselves. Gram-positive bacteria such as Lactococcus , Streptococcus , and Streptomyces spp produce factors, known as bacteriocins, that are another type of AMP and inhibit the growth of other bacterial strains and species that could compete for nutrients and other resources. Staphylococcus epidermidis , the dominant bacterium cultured from the skin microflora, produces another type of AMP, phenol-soluble modulin (PSM)-γ. PSMγ causes membrane leakage in target bacteria, which indicates that they function in a manner similar to that of host-derived AMPs. Interestingly, PSMs are functional in vivo; nanomolar concentrations decreased the survival of group A streptococcus on normal human skin but did not affect the survival of S epidermidis from which the peptide was derived. In addition, PSMs enhance the capacity of bacterial killing activity by human neutrophils by inducing their neutrophil extracellular traps. This implies human innate immune systems cooperate with commensal bacteria to balance the microbiome via those AMPs. Another important example of the protective action of S epidermidis in vivo was observed on the surface of the nasal cavity. Nasal colonization by S aureus was inhibited in individuals who were colonized with specific strains of S epidermidis that produced a serine protease with the capacity to destroy biofilms formed by S aureus . Hence, a thiolactone-containing peptide produced by S epidermidis blocks the S aureus quorum-sensing system that controls the production of various virulence factors. Thus, the selective activity of AMPs produced by commensal organisms may be an important part of a normal host defense strategy against pathogen colonization and microbe-derived AMPs probably work together with host-derived proteins to establish the composition of the skin surface microbiome.
Antimicrobial proteins and human skin disease
Rosacea
The pathogenesis of rosacea is complex. Emotional stress, spicy foods, hot beverages, alcohol consumption, high environmental temperatures, sun exposure, and menopause exacerbate rosacea symptoms such as erythema, rash, and telangiectasia. These findings implied that the external environment would affect rosacea but they are not sufficient or specific to rosacea. In other words, specific intrinsic factors in the host that recognizes and responds to the diverse environmental triggers must be the key to understanding the pathogenesis of rosacea. In innate immunity, the pattern recognition system responds to those environmental stimuli. Triggering the innate immune system normally leads to a controlled increase in cytokines and antimicrobial molecules in the skin, including cathelicidin. Some forms of cathelicidin peptides have a unique capacity to be both vasoactive and proinflammatory. A key to understanding rosacea came with the observation that individuals with rosacea expressed abnormally high levels of cathelicidin in their epidermis. Importantly, the cathelicidin peptide forms found in rosacea were not only more abundant but were also different in molecular weights compared with those in normal individuals. These abnormal cathelicidin peptides promote and regulate leukocyte chemotaxis, angiogenesis, and expression of extracellular matrix components, whereas the types commonly found on normal skin function mostly as antibiotics and have little to no action in inflammation. Normally, active form LL-37 is typically present in neutrophils recruited to infected or injured skin; however, in the case of rosacea patients, LL-37 seems to be generated in the epidermis by an abnormal action of serine proteases. When LL-37 was applied in animal models, it was found to be a potent angiogenic factor and resulted in neovascularization in a rabbit model of hind-limb ischemia. Angiogenesis by LL-37 is mediated by formyl peptide receptor-like 1, a G-protein-coupled receptor expressed on endothelial cells. Moreover, epidermal growth factor receptor signaling, which is in part induced by AMPs, induces vascular endothelial growth factor in epidermal keratinocytes. Yamasaki and colleagues reported that injection of cathelicidin or the enzymes that produce cathelicidin into mice skin resulted in skin inflammation resembling pathologic changes in rosacea. Abnormal production of local serine protease KLK5, which processes cathelicidin peptides from a precursor protein in the epidermis, is a cause for the presence of abundant cathelicidin peptides. This suggests that the abnormally high protease activity found in rosacea patients results in abnormal processing cathelicidin to peptides that induce the characteristic inflammation and vascular changes of rosacea ( Fig. 1 ).
Why do individuals prone to rosacea react with high KLK5 and cathelicidin? A potential explanation for this response can be found by understanding that the innate immune system of the skin is programmed to detect microbes, tissue damage such as ultraviolet (UV)-induced apoptosis, or damage of the extracellular matrix. TLRs are a major and potent mechanism that broadly recognizes microbe derivatives and induces cellular responses such as cytokines and AMPs. In the skin of individuals with rosacea, TLR2 is more highly expressed compared with nonaffected individuals. Increased TLR2 enhances skin susceptibility to specific environmental stimuli and leads to increased cathelicidin production. Cathelicidin transcription in epidermal keratinocytes is also regulated by the active form of vitamin D 1,25(OH) 2 D3. TLR2 stimulation amplifies 1,25(OH) 2 D3 by increasing enzymatic conversion from the inactive form found in the diet and generated by UV exposure. In turn, increased 1,25(OH) 2 D3 enables the epidermis to produce more cathelicidin antimicrobial peptides. KLK5 mRNA transcription is also increased by 1,25(OH) 2 D3 keratinocytes. Actually, increasing or stimulating TLR2 increased KLK5, whereas knocking out TLR2 decreased KLK5. These findings, therefore, suggest that the increase of TLR2 in rosacea skin makes the skin of these patients susceptible to microbes and environmental stimuli, resulting in high cathelicidin and KLK5 expression that then evokes the disease. Interestingly, it is reported that glucocorticoids increase TLR2 expression in epidermal keratinocytes. This may imply that glucocorticoid-induced rosacea-like dermatitis, so-called perioral dermatitis, includes erythema, pustules, and papules somewhat similar to those seen in rosacea, may be caused via TLR2. Finally, many of the current therapies for rosacea can be explained via this pathway. Topical and oral retinoids not only induce connective tissue remodeling but also downregulate TLR2. Azelaic acid decreases the expression of KLK5 and cathelicidin. And doxycycline has anti-inflammatory function via decrease of KLK5 activity by inhibiting matrix metalloproteinases. Recently, Muto and colleagues reported that mast cells (MCs)-deficient (KitW-sh) mice did not develop rosacea-like features after LL-37 injection into the dermis and that stabilization of mast cells can directly reduce skin inflammation in mice and rosacea patients. These results highlight the important role of mast cells in the development of inflammation after cathelicidin activation and the possibility of downregulation of activated mast cells for a therapy for rosacea. In vivo, Two and colleagues described that inhibition of KLK5 may improve the clinical signs of rosacea by decreasing LL-37 production. A turning point of rosacea therapy may have been reached.
Psoriasis
Psoriasis is neither an exclusive epidermal disease nor a pure T-cell–mediated disorder. Clearly, T cell responses are critical, including the contribution of both T-helper (Th)1 and Th17 cells to promote inflammation by producing cytokines, including TNF-α, IFN-γ, interleukin (IL)-12, IL-17A, IL-22, and IL-23. However, epidermal keratinocytes within the epidermis of psoriatic plaques are also abnormal in many aspects and likely influence immunocytes by production of inflammatory cytokines and chemokines. One of the abnormalities of keratinocytes in psoriasis is the excessive production of AMPs. Harder and colleagues isolated human β-defensin (hBD)2 and hBD3, which are only induced by stimulation with proinflammatory cytokines and microbial products, and from psoriatic scales. β-defensin gene copy numbers have been associated with the severity of psoriasis. TNF-α and IFN-γ, which are highly expressed in psoriatic lesions, induce hBD2 and hBD3 expression in keratinocytes. In addition, Th17 cytokines, IL-17A and IL-22 are also inducers of hBD2. The role for hBD in the pathogenesis of psoriasis is not fully understood. However, recently Lande and colleagues reported that hBD2, hBD3, and lysozyme can activate plasmacytoid dendritic cells (pDCs) by themselves and in cooperation with LL-37.
Among the 21 S-100 proteins, S100A7 (psoriasin), S100A8 (calgranulin A), S100A9 (calgranulin B), S100A12 (calgranulin C), and S100A15 have some antimicrobial activity. These are all abundantly expressed in psoriatic lesions or are elevated in serum from psoriatic patients. S100A7, psoriasin, has been best studied because this protein was first discovered in psoriatic skin lesions. This molecule is induced by calcium, vitamin D, retinoic acid, microbial products, TNF-α, IL-17A, and IL-22, and is thought to have a chemotactic role in psoriasis.
Cathelicidin has been highlighted as a modulator of psoriasis development. The upregulation of LL-37 expression in psoriatic epidermis was reported first in 1997. Afterward, it has been shown that the abundance of AMPs including LL-37 and hBD2 in psoriatic lesions is associated with a low rate of infection. In 2007, Lande and colleagues demonstrated an important immune-modulatory function for LL-37 in psoriasis. LL-37 can drive inflammation in psoriasis through its capacity to enable pDCs to recognize self-DNA through TLR9. This response is different from the classical concept that TLR9 recognizes unmethylated DNA sequences (CpG dinucleotides) found in microbial DNA and, in turn, serves as an innate immunity warning system against infection. This activation induces a large amount of type I IFN production, leading to myeloid dendritic cells (mDCs) activation, Th1/Th17 differentiation, and keratinocyte activation. The involvement of type I IFN in the pathogenesis of psoriasis has been suggested by several studies and type I IFNs have been reported to activate autoimmune T cells through the maturation of DCs. pDCs are thought to be major type I IFN-producing cells, and produce many IFN-α in psoriasis ; however, Morizane and colleagues has demonstrated that LL-37 and DNA activation of keratinocytes also greatly increases type I IFN production through TLR9. Therefore, the main source of type I IFNs must be reconsidered again because there are more keratinocytes than pDCs in skin, and because keratinocytes are in more superficial site with greater direct contact to genomic DNA and other external stimuli known to exacerbate inflammation. This may be relevant to the Köbner phenomenon seen in psoriasis, in which clinical exacerbation is caused by minor superficial injury of the epidermis. LL-37 secretion and following IFN production via TLR9 activation may explain this phenomenon. Furthermore, LL-37 has also forms complexes with self-RNA, leading to the activation of TLR7 in pDCs and TLR8 in mDCs in psoriasis ( Fig. 2 ). Moreover, in search of a DC type that specifically accumulates in psoriatic skin lesion and has proinflammatory function, Lowes and colleagues reported on TNF-α and inducible nitric oxide synthase-producing DCs. These cells have the phenotype of CD1c − and CD11c + DCs. They are also referred to as 6-sulfo LacNAc (slan) DCs by the selective expression of the slan residue on the P-selectin glycoprotein ligand 1 membrane molecule. These inflammatory DCs respond to complexes formed of LL-37 and self-RNA via TLR7 signaling and enable Th1/Th17 cells to produce IL-17, IL-22, TNF-α, and IFN-γ more powerfully than classic CD1c + DCs.
Related posts:
 Basic Science Insights into Clinical Puzzles
Basic Science Insights into Clinical Puzzles
 Establishing Tolerance to Commensal Skin Bacteria
Understanding Inherited Cylindromas
Establishing Tolerance to Commensal Skin Bacteria
Understanding Inherited Cylindromas
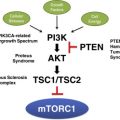 Mosaic Disorders of the PI3K/PTEN/AKT/TSC/mTORC1 Signaling Pathway
Interleukin-22 and Cyclosporine in Aggressive Cutaneous Squamous Cell Carcinoma
Mosaic Disorders of the PI3K/PTEN/AKT/TSC/mTORC1 Signaling Pathway
Interleukin-22 and Cyclosporine in Aggressive Cutaneous Squamous Cell Carcinoma
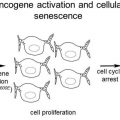 Melanocytic Nevi and the Genetic and Epigenetic Control of Oncogene-Induced Senescence
Melanocytic Nevi and the Genetic and Epigenetic Control of Oncogene-Induced Senescence
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


