The anterolateral thigh (ALT) flap is a popular flap for lower extremity reconstruction despite its varied pedicle anatomy. Beyond its use for soft tissue coverage, using the chimeric flap concept, the ALT flap is useful for tendon and ligament reconstruction and the creation of a gliding surface with the fascia lata component. The vastus lateralis muscle can be included for dead-space obliteration. The main pedicle is long and is a similar size match for major artery reconstruction. If several perforators are available, a split flap could be fashioned into a multitude of shapes all arising from the same pedicle.
Key points
- •
The use of preoperative anterolateral thigh (ALT) flap perforator mapping helps facilitate the design of a skin flap.
- •
There are currently expanding indications for the versatile ALT flap for lower extremity reconstruction.
- •
ALT flap variation allows the incorporation of a chimeric flap design for lower limb defect reconstruction.
- •
It is not only available as a free flap but also can be raised as a pedicled ALT flap to provide a large arc of coverage for soft tissue reconstruction.
- •
ALT flap with 2 or more perforators can be used as split flaps or several independent flaps.
Introduction
The anterolateral thigh (ALT) flap is one of the most versatile flaps in a reconstructive surgeon’s armamentarium. It is considered one of the more contemporary flaps in this era as reconstruction preferences change throughout the times. Its variations in design and tissue components in terms of a fasciocutaneous or chimeric flap with multiple components, including muscle and fascia, serve to reconstruct a myriad of defects. The ALT flap also has a lower donor site morbidity and can be harvested in the supine position, obviating any position change, which is convenient for most procedures.
In lower extremity reconstruction, gaining optimal coverage quickly and safely is only the basic function of an ALT flap. The main pedicle, termed the descending branch of the lateral circumflex femoral artery (LCFA) and vein, allows a long and similar size match in vessel reconstruction of the lower limb. The various tissue types in the lower limb can be replaced with similar tissues in the ALT flap, which can be harvested with skin and fat alone or with muscle, fascia, and bone together. Volume for dead-space obliteration can be easily performed with the ALT flap. The fascia lata included in the ALT flap can be rolled to replace tendinous gaps in the lower extremity, such as the Achilles tendon. The iliac crest bone attached to the ALT flap or tensor fascia lata could be harvested simultaneously for 1-stage lower leg open fracture reconstruction that requires both soft tissue and bone components.
Indications and contraindications
The ALT flap is indicated when there is a need for large surface area or volume defect reconstruction with vascularized tissue in the lower extremity. When recipient vessels are a distance away, the ALT flap can be used with a long pedicle and large flap based on a distal perforator for greater length. The ALT flap is also a good option when multiple tissue types are required. It is an ideal flap for its versatility of inset and components that can be used to replace missing tissue for several purposes, including dead-space obliteration, the creation of a tendon gliding surface, tendon or ligament reconstruction, 1-stage soft tissue and bone defect reconstruction, a flow-through flap for major artery reconstruction, for coverage of a functioning rectus femoris muscle flap, or even for aesthetic soft tissue augmentation.
However, the contraindications are the same as for any free flap, including patients with severe comorbidities, extensive atherosclerotic disease, and a dirty wound bed. When the donor site has been used before leaving no proximal stump of the descending branch of the lateral circumflex femoral vessels, the ALT flap should not be attempted. The ALT flap is also not preferred when extensive scar formation on the territory of the ALT flap is seen either from previous surgery or from trauma.
Preoperative evaluation and special considerations
Preoperative Perforator Mapping
Handheld Doppler preoperative determination of perforators is generally reliable in the ALT flap, but they can vary in location during dissection. Computed tomography (CT) angiography for ALT flap perforator mapping is useful for chimeric flap design but is not always necessary in experienced hands because of concern of radiation exposure and resource consumption. Duplex ultrasonography is now another useful noninvasive choice for preoperative assessment of pressure and diameter of the perforators as well as their flow rate and course, which aids in dissection and flap design.
Split Anterolateral Thigh Flap
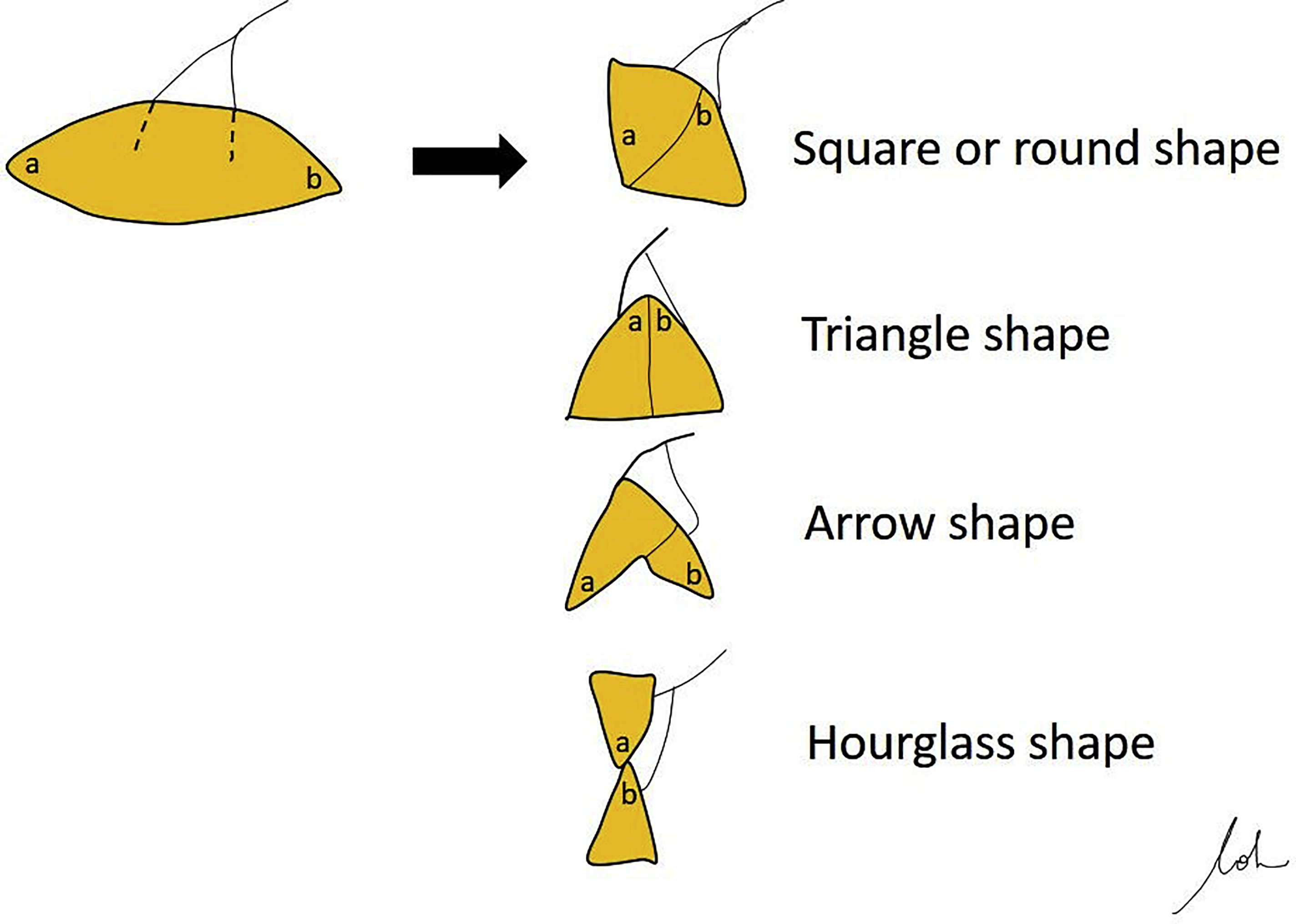
The ALT flap can be split into various flaps depending on the perforators included in the flap. As such, this flap can be fashioned into a multitude of shapes all arising from the same pedicle, facilitating efficient use of the flap , ( Fig. 1 ).
One Donor Site, 2 or more Free Flaps
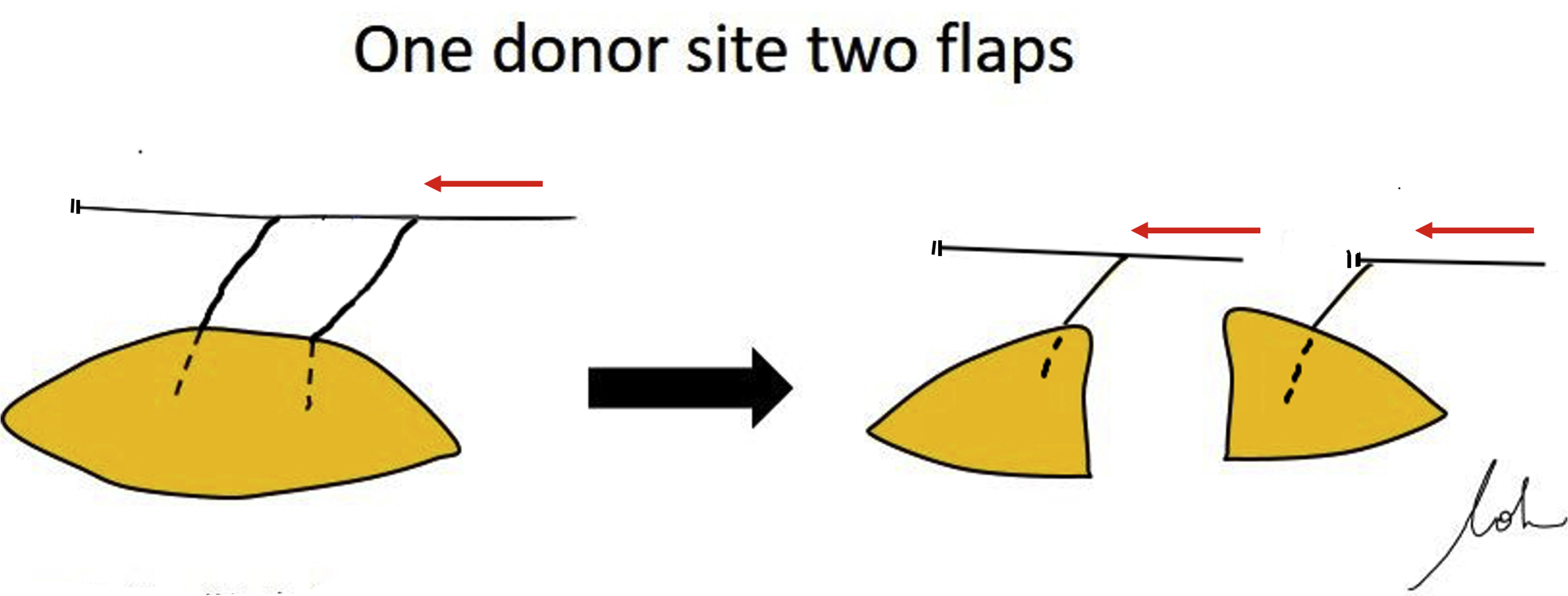
The length of the descending branch of lateral circumflex also allows division of 1 ALT flap into 2 or more ALT flaps, each with its own separate perforators. The trick is ligation of the main trunk immediately distal to the bifurcation of the proximal perforator to get longer pedicle length for the distal flap. These techniques all allow minimizing donor site morbidity and maximizing flap output from a single donor site, which is not always possible with other flaps ( Fig. 2 ).
Timing of Flap Reconstruction
Marko Godina established the principle of early flap coverage for traumatic lower extremity injuries. Early free flap coverage performed within 3 days of injury has a lower flap failure rate and infection rate than the delayed free flap reconstruction (4–90 days) group. Based on a retrospective review of 358 free flap reconstructions, Lee and colleagues updated Godina’s paradigm, and the ideal early flap reconstruction can be safely performed within 10 days of injury without an adverse effect on outcomes. Reconstruction at an early stage has the benefit of less scarring and fibrosis around the vessels, which can make it more difficult for vessel dissection and lumen expansion. However, patients with trauma may present to the reconstructive surgeon at any time after their injury or after their earlier unsuccessful reconstruction, hence, surgeons should not be confined by those time lines. In our experience, timing may not be that critical, provided the surgeon is knowledgeable about time-related pathophysiology of the damaged tissue and is able to perform adequate debridement. A high flap success rate can still be expected even in the subacute phase. Immediate emergency flap reconstruction is defined as simultaneous flap coverage performed immediately following debridement after injury. It is indicated in cases where cover over an exposed critical organ (vessel, nerve, tendon, or bone) is required or to create a flow-through revascularization of the limb at the same time. Adequate debridement is the key point to achieving success in immediate emergency flap reconstruction.
Surgical procedures for expanding indications
Dead-Space Obliteration
The presence of dead space can be filled with fluids that are easily infected. The ALT skin flap itself or vastus lateralis (VL) muscle can be used to fill large defects and obliterate dead space. The VL muscle is often supplied by the muscular branches of the same descending branch of the lateral circumflex pedicle. , The design with separated skin paddle and a VL muscle part could increase the flap inset freedom and avoid inadvertently damaging the perforator during its harvest, especially when the muscle is cut to the appropriate size. If further bulk is required, deepithelialization of the skin paddle can be performed and tucked into the defect. Inserting of drains into the dead space that is to be obliterated helps reduce any buildup of fluids, which can be a nidus of infection and compromise vascularity of the flap postoperatively ( Fig. 3 ).
Creation of Tendon Gliding Surface
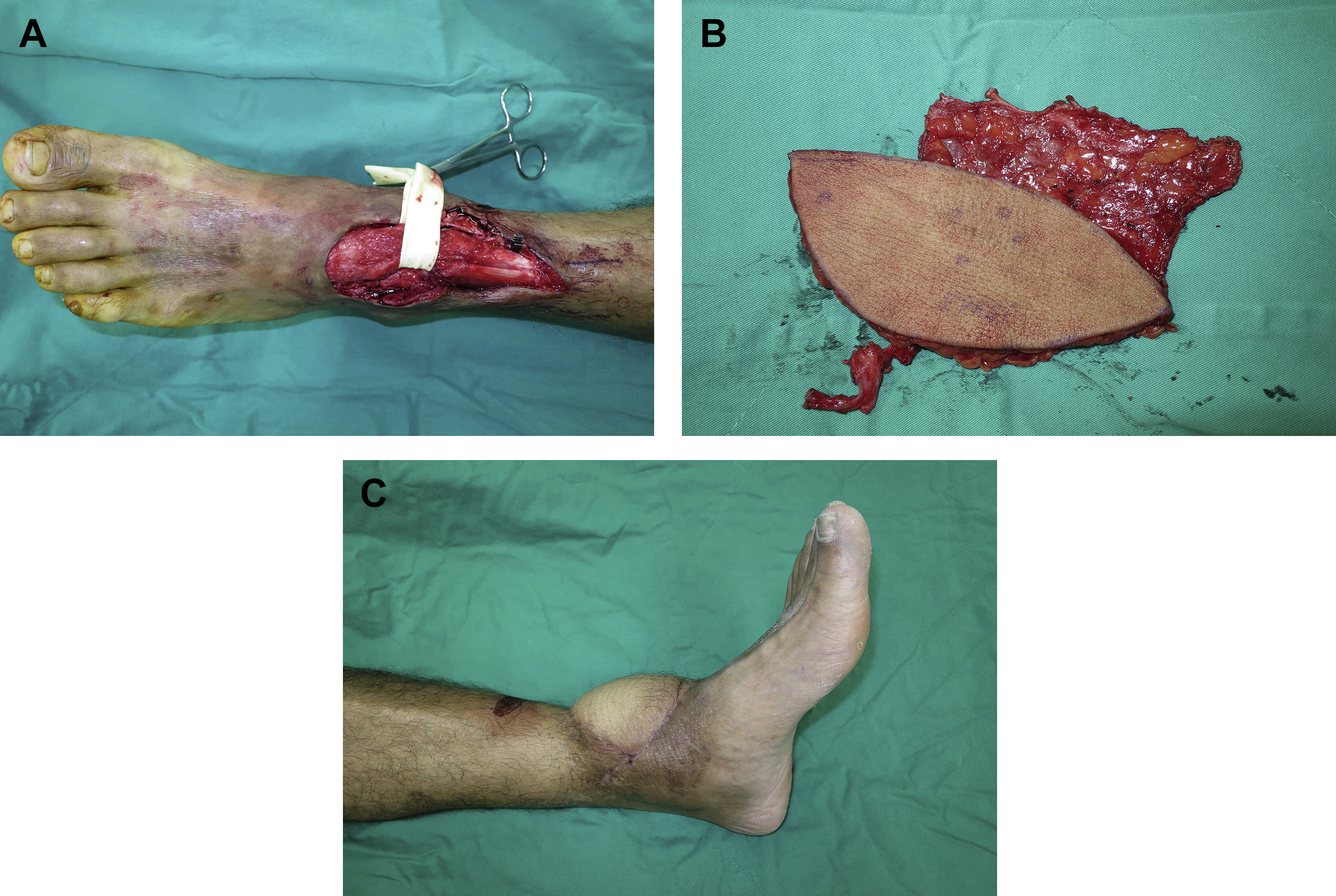
Tendons are unique because they serve a function that requires them to glide with the excursion of their respective muscle bellies. Skin grafting onto exposed tendon is also not feasible in most cases because take is not guaranteed, especially with denuded paratenon. The other problem with skin grafting onto tendons is that the graft is adherent and scars up, causing the tendons to stick and in turn reduce their function without appropriate glide and excursion. As such, the fascial component of an ALT fasciocutaneous flap that is vascularized can act as a barrier on top of the exposed tendons to minimize adhesions formed postoperatively. This approach in turn reduces the need for subsequent tenolysis to achieve a desirable function ( Fig. 4 ). This ALT fasciocutaneous flap harvest can be designed in a more lateral aspect of the regular ALT territory to include a larger piece of fascia lata.
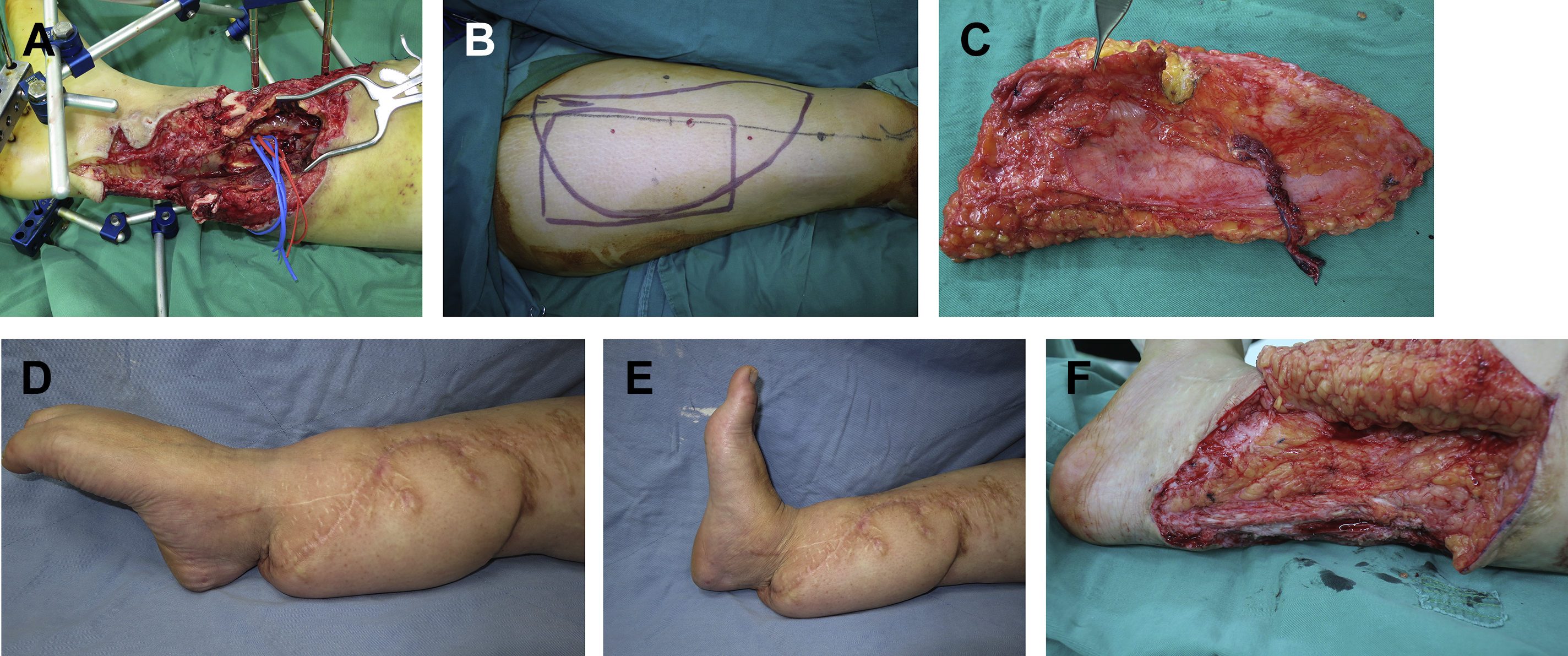
Tendon or Ligament Reconstruction
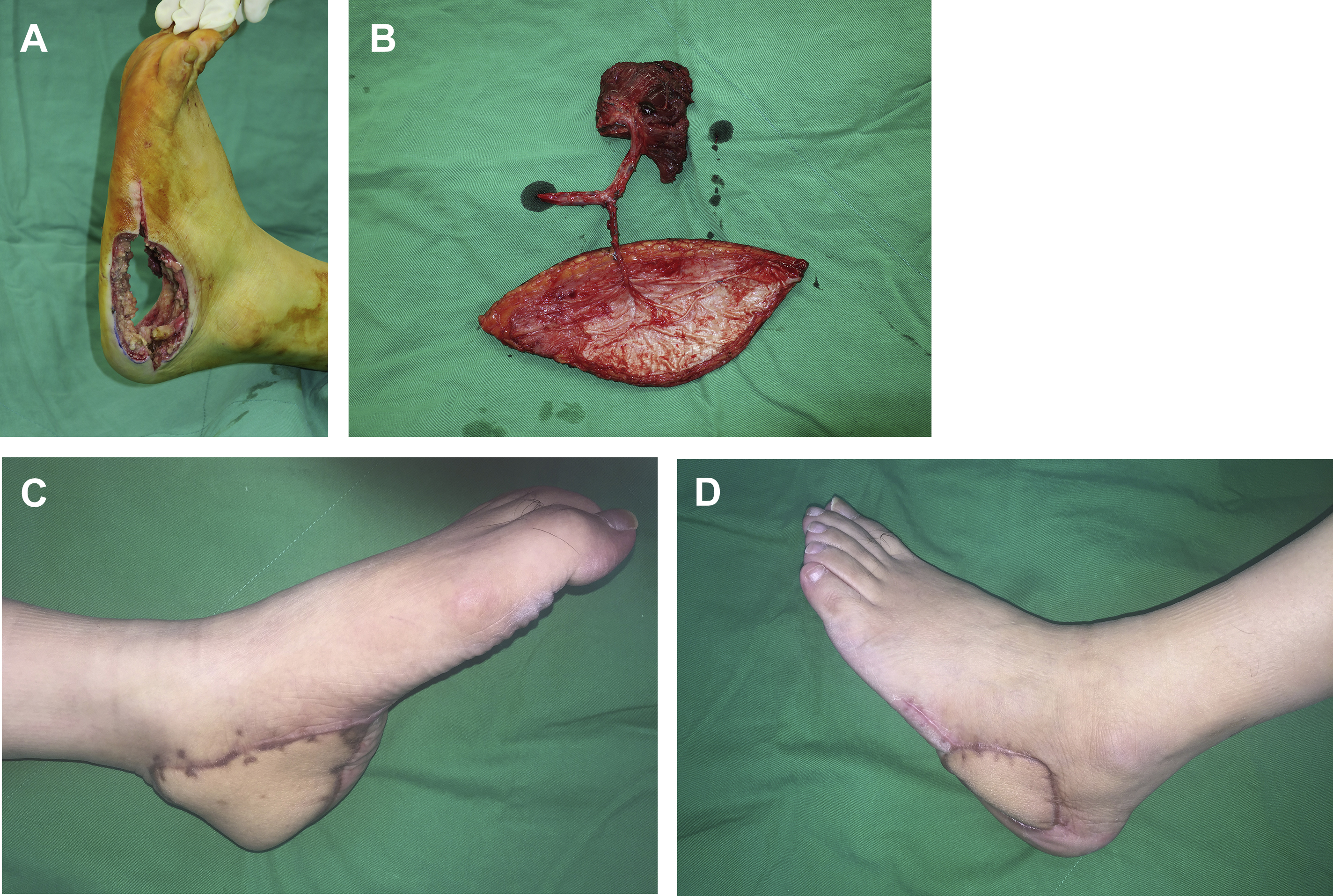
The fascia lata component of the ALT flap (ALT fasciocutaneous flap) can be rolled to form a tendonlike structure for large tendon defect reconstruction. It can be used for reconstructing the anterior tibialis and the Achilles tendon in the lower extremity. Planning with a template to design the ALT flap in the position of the pedicle and length of the fascia lata for tendon reconstruction has to be done preoperatively because the rolled fascia has to be placed under the optimal tension and right orientation to prevent pedicle compression by the reconstructed tendon. The fascia remains revascularized and bleeding when the flap is debulked at a later stage. Full restoration of ankle movement is also possible with this technique ( Fig. 5 ). The patellar ligament and anterior tibialis tendon are crucial for knee and ankle extension and can also be reconstructed with an ALT fasciocutaneous flap with rolled fascia ( Fig. 6 ).
Related posts:
 Propeller Flaps in Lower Extremity Reconstruction
Propeller Flaps in Lower Extremity Reconstruction
 The Medial Sural Artery Perforator Flap in Lower Extremity Reconstruction
The Medial Sural Artery Perforator Flap in Lower Extremity Reconstruction
 Free-Style Free Perforator Flaps in Lower Extremity Reconstruction
Free-Style Free Perforator Flaps in Lower Extremity Reconstruction
 Microsurgical Reconstruction of the Lower Extremity in the Elderly
Microsurgical Reconstruction of the Lower Extremity in the Elderly
 Orthoplastic Approach to Lower Extremity Reconstruction
Orthoplastic Approach to Lower Extremity Reconstruction
 Lower Extremity Reconstruction in the Pediatric Population
Lower Extremity Reconstruction in the Pediatric Population
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


