CHAPTER 12 The Anterolateral Minimal/Limited Incision Intermuscular Approach





PREOPERATIVE PLANNING
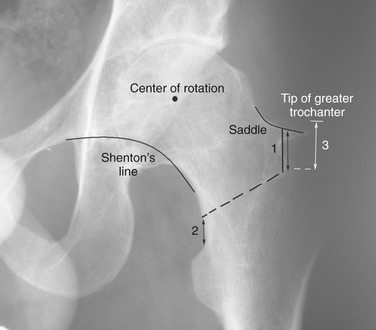
Preoperative templating is performed on anteroposterior radiographs of the pelvis and on a lateral view of the hip. The specific objectives of preoperative planning include calculation of any leg length discrepancy and restoration of appropriate femoral offset, and determination of component sizes. Three important measurements are taken to aid intraoperative decision making for the femoral osteotomy and seating of the component (Fig. 12-1). The first measurement is the distance from the saddle of the neck (the superior surface of the femoral neck at the base of the medial face of the greater trochanter) to where the definitive osteotomy is to be performed. The second measurement is the distance from the lesser trochanter to the medial point of the femoral osteotomy. The last measurement is from the tip of the greater trochanter to the shoulder of the prosthesis in its final location. Strict adherence to these measurements allows precise placement of components with minimal error and without compromising of stability.