Tenzel Semicircular Rotational Flap
John Nguyen
Aaron Fay
DEFINITION
It is conceptually similar to the classic Mustarde cheek rotation flap but provides better dynamic reconstruction of the various eyelid lamellae with less tissue rearrangement.
The Tenzel flap utilizes the rotation of a semicircular musculocutaneous flap beginning at the lateral canthus, extending either downward (for upper eyelid reconstruction) or upward (for lower lid reconstruction) to close full-thickness defects of the eyelid ranging from one-third to two-thirds of the horizontal length of the eyelid margin.
Both the anterior lamella (skin and orbicularis muscle) and the posterior lamellar (tarsus and conjunctiva) are addressed in a single-stage operation. The final postoperative appearance of the flap is superior to skin grafting or the larger Mustarde flap.4
A large defect up to two-thirds of the horizontal length of the lower eyelid can be repaired with the Tenzel semicircular flap.
ANATOMY
The upper and lower eyelids meet at the lateral canthus, a tendon-ligament complex that is firmly attached to Whitnall tubercle, 2 to 4 mm deep to the lateral orbital rim. The anterior eyelid lamella (skin and orbicularis oculi) is continuous in this region.
The thin eyelid skin transitions to thicker facial skin that contains subcutaneous fat, and the orbicularis oculi extends approximately 2.5 cm beyond the lateral orbital rim.
Posteriorly, the suborbicularis oculi fat lies anterior to the periosteum of the zygomatic bone.
The periosteum of the orbit (periorbita) and zygomatic bone condense at the orbital rim to form the arcus marginalis; the strong periosteum can be useful to provide elevation support for the flap (FIG 1A,B).
Arterial supply is derived from the lacrimal artery, giving rise to the zygomaticotemporal artery, exiting the lateral orbital wall at midorbit, and to the zygomaticofacial artery, running inferolaterally to exit through a small foramen in the zygomatic bone.
Both the zygomaticofacial nerve and the zygomaticotemporal nerve arise from the maxillary nerve.
The zygomaticofacial nerve leaves the orbit inferolaterally through the zygomaticofacial foramen along with the artery and supplies the skin of the malar eminence.
The zygomaticotemporal nerve similarly egresses the zygomatic bone superiorly to supply the anterior temple (FIG 1C,D).
PATIENT HISTORY AND PHYSICAL FINDINGS
Eyelid defects occur most commonly from trauma or tumor resection. Other causes include burns and congenital abnormalities.
Basal cell carcinoma is the most common eyelid malignancy (90%); squamous cell carcinoma, sebaceous cell carcinoma, and cutaneous melanoma are neoplasms that involve the eyelids in order of decreasing frequency.
The biologic behavior of the tumor should be a key consideration in reconstructing a large eyelid defect as it can affect long-term prognosis.
Factors such as the size and orientation of the defect, patient age, vascular supply to surrounding tissues, previous treatment (both surgical and radiation), and age of the wound should also be carefully assessed, as any of these can affect surgical plan and outcome.
The Tenzel flap is most useful when there is sufficient lateral canthal skin laxity and there is at least a small portion of the full-thickness eyelid available on either side of the defect.
It can be used when there is no tarsus on the lateral side of the defect, but optimal results will require a periosteal flap or tarsal replacement graft such as hard palate mucosa, auricular cartilage, nasal septal chondromucosal graft, free tarsoconjunctival graft, allograft, or xenograft to provide the stability that is normally provided by the tarsus.
Without proper structural support, the lateral portion of the eyelid is likely to roll inward, causing chronic ocular surface injury.
In cases of irradiation or burn injury, the Tenzel flap is preferred over grafting as the flap provides its own vascular supply.
NONOPERATIVE MANAGEMENT
In general, significant eyelid defects require surgical repair.
Nonoperative management of large eyelid defect can lead to eyelid notching, scarring, entropion, ectropion, trichiasis, and lagophthalmos with corneal exposure causing corneal injury, infection, eyeball rupture, and blindness.
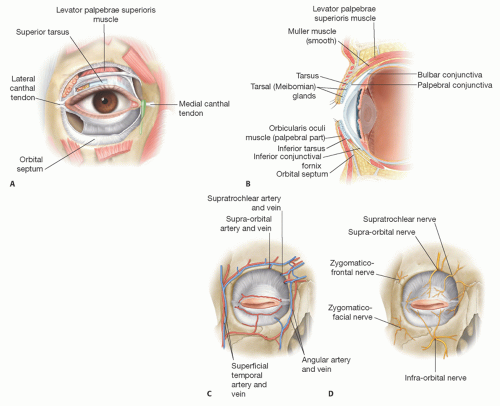 FIG 1 • Anatomy (A,B), blood supply (C), and sensory nerve innervation (D) of the eyelids. |
Related posts:
 Mandible Reconstruction With Fibula Flap With Templates
Mandible Reconstruction With Fibula Flap With Templates
 Lower Lip Reconstruction With the Nasolabial Flap
Lower Lip Reconstruction With the Nasolabial Flap
 Lower Eyelid Reconstruction With Palatal Grafts
Lower Eyelid Reconstruction With Palatal Grafts
 Reconstruction of the Ear Lobe
Reconstruction of the Ear Lobe
 Pectoralis Major Flap for Pharyngeal Reconstruction
Pectoralis Major Flap for Pharyngeal Reconstruction
 Facial Reanimation in the Oncologic Patient Using Nerve Grafts and Nerve Transfers
Facial Reanimation in the Oncologic Patient Using Nerve Grafts and Nerve Transfers
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


