Temporo-Parietal Fascial Flap to Cover “Silastic” Framework in Ear Reconstruction
S. OHMORI
In employing Cronin’s technique using a silicone frame in the repair of microtia (1), I found that the mastoid needed to be excavated to house the concha (created by a silicone prosthesis). The overlying flap must be created in such a way that no tension is produced. I used the method on 87 patients, and follow-up study showed that although a fairly deep concha could be created by this method, minor fistulas developed in 25 sites in the area where the L-shaped incision was made (Fig. 96.1). These fistulas led to infection, which necessitated removal of the silicone frame in nine of 87 reconstructed ears. The incidence of removal was considerable enough to make one hesitate to adopt the silicone frame (2, 3, 4). The temporoparietal fascial flap can resolve this problem.
INDICATIONS
The temporoparietal fascia is brought to the conchal part of the silicone frame and anchored to the surrounding skin. The concha is made deeply concave, and the helix becomes clearly visible. The fascia then is skin-grafted. Because there is no tension over the frame, fistula formation is less likely. The fascia is thin, has an excellent blood supply, and leaves no functional donor defect.
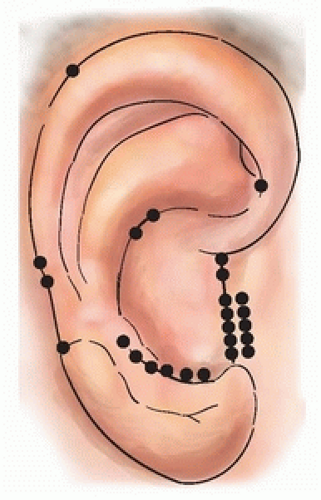 FIGURE 96.1 Minor exposure of the frame was found mostly along the L-shaped incision scar, proving that there is a shortage of skin in the flap that covers the frame. The dots show the sites that have been exposed in the past. (From Ohmori, Matsumoto, ref. 2, with permission.) |
FLAP DESIGN AND DIMENSIONS
Preoperatively, the course of the superficial temporal artery is marked on the temporal skin using palpation or the Doppler probe (Fig. 96.2A). During the operation, a T-shape is drawn, following the marked course of the artery (Fig. 96.2B). A line of 5.5 to 6.0 cm in length is drawn at a distance of 7.5 to 8.0 cm from the hairline.
Related posts:
 Cheek Rotation Skin (Mustardé) Flap to The Lower Eyelid
Cheek Rotation Skin (Mustardé) Flap to The Lower Eyelid
 Nasalis Musculocutaneous Sliding Flaps for Nasal Tip Reconstruction
Nasalis Musculocutaneous Sliding Flaps for Nasal Tip Reconstruction
 Inferior Turbinate Flap for Closure of Septal Perforations
Inferior Turbinate Flap for Closure of Septal Perforations
 Postauricular and Retroauricular Scalping Flap (The Paras Flap)
Postauricular and Retroauricular Scalping Flap (The Paras Flap)
 Scapular and Parascapular Flaps
Scapular and Parascapular Flaps
 Platysma Musculocutaneous Flap to The Lower Lip
Platysma Musculocutaneous Flap to The Lower Lip
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


