Temporalis Flap and Lengthening Temporalis Myoplasty for Facial Paralysis
Andre Panossian
DEFINITION
Facial paralysis is the result of facial nerve dysfunction (cranial nerve VII). It can be congenital or acquired, bilateral or unilateral. Patients with facial paralysis exhibit drooping of the lower face and loss of lip closure/elevation.
Muscle transfers are indicated in cases of long-term, or permanent, facial paralysis (greater than 18 months).
Regional or free muscle transfer can restore unidirectional movement of the lips and lower face by using branches of the contralateral facial nerve or unaffected ipsilateral cranial nerves (eg, trigeminal nerve branches for mastication [V3]).
The temporalis flap is a procedure for transferring the function of the ipsilateral temporalis muscle in a retrograde, or “turnover,” fashion to the lips and oral commissure for the purpose of reanimating the lower face. The methods outlined herein include further refinements to the techniques originally developed by Gillies.
The lengthening temporalis myoplasty is a procedure for reorganizing and transferring the function of the ipsilateral temporalis muscle in an orthodromic fashion to the lips and oral commissure for the purpose of reanimating the lower face. The methods outlined herein include further refinements to the techniques originally developed by McLaughlin1 and refined by Labbé.2,3
ANATOMY
The temporalis is one of four muscles of mastication (innervated by cranial nerve V). It is a broad muscle that originates in the temporal fossa and inserts onto the coronoid process of the mandible.
The temporalis consists primarily of two layers, deep and superficial, that converge onto a single tendon (FIG 1A). The tendon is broad and wraps around the coronoid process in a conical fashion, extending down onto the ramus for several millimeters.
The muscle is dually innervated at the infratemporal crest by the deep temporal nerves (from the mandibular division of the trigeminal nerve V3). It also has dual circulation from the deep temporal arteries (branching from the maxillary artery) (FIG 1B).
Muscle fibers from the masseter and the pterygoids attach to portions of the temporalis tendon as it passes through the zygomatic, or infratemporal, fossa.
PATHOGENESIS
There are numerous causes of facial paralysis that are broadly classified as congenital or acquired.
The most common form is acquired complete unilateral facial nerve palsy of an inflammatory etiology (ie, Bell palsy). Although most cases will resolve spontaneously, a small number of patients will continue to experience persistent facial paralysis or weakness causing noticeable asymmetry of function and appearance.
The cause of a patient’s paralysis must be investigated in order to direct treatment and estimate prognosis for recovery.
PATIENT HISTORY AND PHYSICAL FINDINGS
Preoperative evaluation of patients with facial paralysis includes a detailed history and assessment of the patient’s current facial nerve function and secondary deformities.
History
Etiology (trauma, viral, tumor, syndromic, etc.). It is important to determine whether the cause is congenital or acquired.
Associated symptoms (vertigo, tinnitus, vision changes, ataxia, apraxia, symptoms related to other cranial nerve palsies, stroke, etc.)
Treatments administered to date (radiation, slings, canthoplasty, muscle flaps, etc.)
Unilateral vs bilateral and complete vs partial facial paralysis
Time course
Early: less than 12 months
Intermediate: 12 to 18 months
Late: greater than 18 months
Physical examination is used to determine the location and extent of facial paralysis and resulting deformities. In addition, physical examination should document function of other cranial nerves and assess potential causes of facial paralysis (if possible).
For assessment of facial paralysis and its sequela, the face is divided into thirds.
Upper third: Paralysis of the upper face results in brow ptosis, lack of forehead rhytides, and compensatory contralateral forehead elevation.
Middle third: Middle third paralysis results in incomplete eyelid closure with lower lid malposition (lagophthalmos and ectropion). The physical examination should document Bell phenomenon (a defensive movement of the eye that is present in most patients resulting in upward movement of the eye with eye closure) and reliance on eye lubricants. In addition, symptoms of epiphora and dry eyes should be elicited.
Lower third: Lower third paralysis results in mouth droop, drooling, loss of or asymmetric smile, pucker, articulation, and lower lip depression
Smile assessment
Loss of nasolabial fold: Patients with partial facial paralysis will have partial loss or asymmetric nasolabial folds.
Contralateral deflection of the lips, accentuated with smiling (negative vector of excursion)
Incomplete bilabial closure
Record vector direction and length of oral commissure excursion of paralyzed and nonparalyzed sides (may be a negative number).
Examination and documentation of remaining cranial nerve function particularly function of the fifth cranial nerve. This can be done simply by assessing temporalis and masseter muscle function when biting down.
Diagnostic studies
Brain MRI is sometimes indicated to rule out tumor etiology or secondary compression.
Although nerve conduction studies may be helpful in treatment planning for facial paralysis patients in the intermediate term, they are of limited use in patients experiencing permanent or long-standing facial nerve palsy.
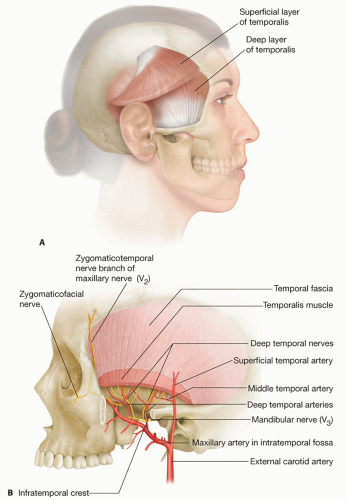 FIG 1 • A. The temporalis muscle consists primarily of superficial and deep layers. B. Dual neurovascular supply of the temporalis muscle. Deep temporal nerves derive from the mandibular division of the cranial nerve (V3), and deep temporal arteries branch from the maxillary artery. |
IMAGING
Brain MRI or CT scans are occasionally needed when an intracranial mass or vascular malformation is suspected.
In patients with long-standing (or, late) facial paralysis with proper early workup, diagnostic studies are rarely indicated in order to proceed to surgery.
SURGICAL MANAGEMENT
Retrograde temporalis flap
Temporalis flap is a retrograde, or “turnover,” muscle transfer that passes over the zygomatic arch, using the contraction produced by the temporalis.
There are several versions of the retrograde temporalis flap for facial paralysis. We describe the traditional version with modifications herein.
Candidates for a traditional temporalis flap exhibit permanent facial paralysis (greater than 18 months) with either no anticipated recovery or inadequate recovery.
Unilateral or bilateral temporalis flaps may be performed simultaneously.
Risks include temporal hollowing, adhesions, loss of mobility, excessive cheek bulk, unfavorable scarring, persistent asymmetry, and unusual facial dimpling.
Lengthening temporalis myoplasty
Lengthening temporalis myoplasty is an orthograde, or orthodromic, muscle transfer deep to the zygoma, using the natural direction of pull produced by the temporalis (FIG 2).
Candidates for lengthening temporalis myoplasty exhibit permanent facial paralysis (greater than 18 months) with either no anticipated recovery or inadequate recovery.
Minimum age for procedure is approximately 5 years.
Unilateral or bilateral temporalis myoplasties may be performed simultaneously.
Risks include neurovascular injury to the temporalis muscle being transferred, avulsion of the tendon from the implantation site, temporal hollowing, adhesions, loss of mobility, unfavorable scarring, persistent asymmetry, and unusual facial dimpling.
Revision of the insertion site at the nasolabial fold may be required if there is loss of motion postoperatively.
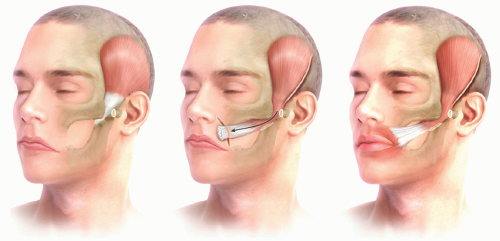 FIG 2 • Concept of lengthening temporalis myoplasty as an orthodromic muscle transfer. |
Preoperative Planning
Mark the location of the desired nasolabial fold (use unaffected side for symmetry, if unilateral). Patient must be able to participate in order to identify accurately the position of the nasolabial fold. In bilateral cases, the location is determined by digital manipulation of the upper lip skin to simulate a smile, thereby identifying the junction between cheek and lip (FIG 3A).
Mark the direction or vector of excursion of the smile at the oral commissure and mid upper lip on the unaffected side and replicate for paralyzed side (FIG 3B).
Positioning
Place the patient in supine position with shoulder roll to gently extend the neck.
A standard endotracheal or armored tube is sutured orally in the midline, making sure there is no tension on the lips.
Prep the entire head and neck, including oral and nasal passages, with diluted iodine or other prep solution.
Inject 1:500 000 to 1 000 000 dilution of epinephrine solution in tumescent fashion over the temporalis muscle and midface. Avoid use of local anesthetic solution to prevent paretic effect on the temporalis muscle.
Approach
Coronal and nasolabial fold incisions are outlined and confirmed. The dissection of the temporalis muscle is the first step.
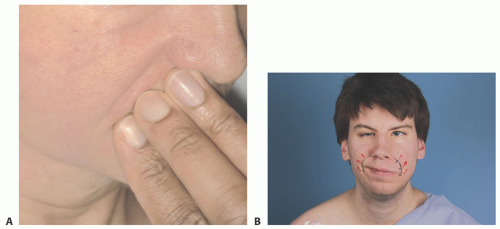 FIG 3 • A. Demonstration of the nasolabial fold simulated with posteriorly directed pressure of the upper lip skin. B. Preoperative facial markings of the intended nasolabial fold and vector of excursion as mirrored from the contralateral side. |
TECHNIQUES
▪ Temporalis Flap
Dissection
Place a coronal anterior hairline incision from the ipsilateral parietal area, converging to a preauricular (facelifttype) incision.
Alternatively, a coronal incision (without preauricular incision) may be used in conjunction with a nasolabial fold counterincision. The nasolabial fold is verified, and key points are tattooed with gentian violet and a 25-gauge needle (TECH FIG 1A).
Make the marked incisions, and elevate the anterior and posterior skin flaps in a deep subcutaneous plane. The plane must proceed along the superficial layer of the deep temporal fascia, preserving an unnamed fat pad over the anterior and inferior portion of the dissection.Related posts:
 Mandible Reconstruction With Fibula Flap With Templates
Mandible Reconstruction With Fibula Flap With Templates
 Lower Lip Reconstruction With the Nasolabial Flap
Lower Lip Reconstruction With the Nasolabial Flap
 Lateral Tarsal Strip Canthoplasty
Lateral Tarsal Strip Canthoplasty
 Antia-Buch Flaps for Ear Reconstruction
Antia-Buch Flaps for Ear Reconstruction
 Reconstruction of Buccal Mucosal Defects
Reconstruction of Buccal Mucosal Defects
 Facial Reanimation in the Oncologic Patient Using Nerve Grafts and Nerve Transfers
Facial Reanimation in the Oncologic Patient Using Nerve Grafts and Nerve Transfers

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


