Most fractures are managed nonoperatively. Those displaced unstable fractures require percutaneous fixation of single (or double) intramedullary Kirschner wires. Only large, oblique fractures must be fixed with screws or a plate. Indications for plating metacarpal fractures are limited in multiple unstable shaft or oblique fractures. After internal fixation, the patient actively moves the digits over a limited range under protection. This article reviews indications and techniques of surgical treatment, hardware removal, and the wide-awake approaches for surgery of these fractures.
Key points
- •
Metacarpal fractures are mostly treated with cast or plaster splint immobilization for 5 to 6 weeks after closed reduction. If the reduction is unstable, percutaneous insertion of single (or double) intramedullary Kirschner wires is an easy and minimally invasive solution for most of these cases.
- •
Only large, oblique fractures may have to be fixed with 1 or 2 screws or a plate. Multiple fractures in the shaft or oblique fractures in multiple metacarpals may need plate fixation as well. Indications for plating metacarpal fractures are very limited.
- •
After internal fixation, the authors advocate early intermittent active motion. The patient actively moves the metacarpophalangeal joint fully, or over a limited range, with a protective plaster splint or with finger buddy taping. The Kirschner wire is removed after bone healing (ie, 4–6 weeks after surgery). Screws and plates may not be removed, but if removal is necessary, it should be done 6 months after surgery.
- •
The wide-awake approach is applicable to internal fixation and hardware removal in fractured metacarpals.
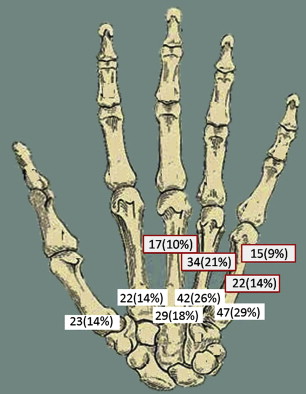
The authors’ hand surgery unit handles 150 to 200 metacarpal fractures each year. Review of upper extremity fractures shows that 163 metacarpal fractures were treated by the authors in 2012. These metacarpal fractures accounted for 7.8% of the all upper extremity fractures or 21.6% of all fractures in the hand (including fractures of carpal bones) ( Fig. 1 ). In the literature, fractures of the metacarpals are reported to account for 18% of fractures below the elbow. The metacarpals of the ring and small fingers are most often involved and fractures occur at the shaft most frequently ( Table 1 ). Cause of the fractures varies greatly. The authors see that most fractures are caused by punching something hard, by machines or tools, or during fighting or sports activities. Pain is the most common complaint. Swelling and limitation in hand motion are common. Plain radiographs are usually sufficient to confirm the diagnosis and assess displacement of the fracture. The radiographs should routinely include posteroanterior, lateral, and oblique views of the affected hand.
| Fracture Locations | Thumb | Index | Middle | Ring | Little | Total |
|---|---|---|---|---|---|---|
| Head | 2 (1.2%) | 2 (1.2%) | 2 (1.2%) | 1 (0.6%) | 2 (1.2%) | 9 (5.5%) |
| Neck | 1 (0.6%) | 5 (3.1%) | 6 (3.7%) | 4 (2.5%) | 15 (9.2%) b | 31 (19.0%) |
| Shaft | 12 (7.4%) | 11 (6.7%) | 17 (10.4%) b | 34 (20.9%) b | 22 (13.5%) b | 96 (58.9%) |
| Base | 8 (4.9%) | 4 (2.5%) | 4 (2.5%) | 3 (1.8%) | 8 (4.9%) | 27 (16.6%) |
| CMC joint | 7 (4.3%) | 2 (1.2%) | 2 (1.2%) | 2 (1.2%) | 5 (3.1%) | 18 (11.0%) |
| Total | 23 (14.1%) | 22 (13.5%) | 29 (17.8%) | 42 (25.8%) | 47 (28.8%) | 163 |
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


