Introduction
As dermatologic surgeons, we can employ a wide variety of approaches to help improve existing scars with more cosmetically pleasing ones. A successful scar revision can markedly improve form, function, and quality of life for these patients. Scar formation is a normal and necessary process for the healing of tissue after insult. However, abnormal healing or disturbed collagen production can result in an inadequate restoration of the cutaneous surface and permanent textural irregularities. A scar generally achieves a steady state after 1 year and will ultimately reach only 80% of the tensile strength of normal skin.
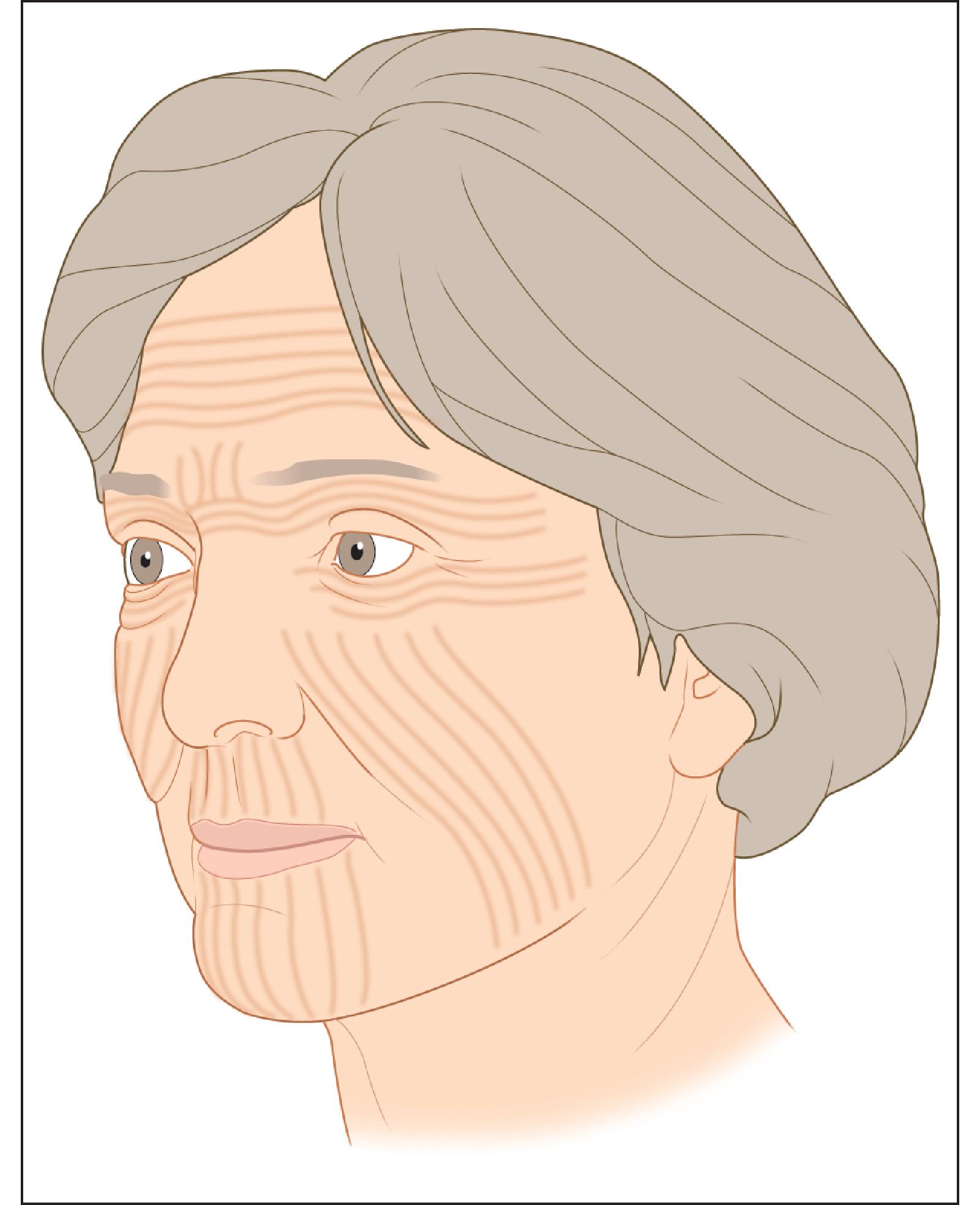
Clinically, a cosmetically acceptable scar is barely perceptible and shares features that are similar to normal skin. These include a scar that is narrow, soft, and level with the surrounding skin. Favorable lines of closure are often hidden along the borders of cosmetic subunits and within or parallel to relaxed skin tension lines (RSTLs), lines due to the dynamic action of the underlying musculature ( Fig. 3.1 ). Preoperative planning and prevention are critical to achieving scar cosmesis. Moreover, a clear understanding of the types of abnormal scars a dermatologist may face and the arsenal of surgical approaches to revise them are of immense benefit in the battle against “ugly” scars.
This chapter will focus on surgical methods for scar revision; however, the authors generally employ a multimodality approach to improving scars. The dermatologic surgeon should be aware that these surgical procedures are usually paired with other treatments such as laser or other adjunctive therapies. For information on the use of lasers and other adjunctive therapies in scar revision, please refer to the appropriate sections of this volume.
Types of Clinical Scars
From an etiologic perspective, there are four main categories of scars that may require revision: (1) poorly designed; (2) traumatic; (3) poorly healed; and (4) disease related ( Table 3.1 ). The resulting scar abnormalities guide the choice of revision techniques ( Table 3.2 ).
| Category | Examples of Causes |
|---|---|
| Poorly designed | Not parallel or within relaxed skin tension lines |
| Lack of respect for facial landmarks | |
| Long linear design | |
| Depressed scars from lack of evertional closure | |
| Traumatic or irregular | Burn |
| wound creation | Debris |
| Prior poor healing | Infection |
| Excess tension | |
| Necrosis or slough | |
| Disease related | Acne |
| Varicella | |
| Keloid |
| Scar Abnormality | Causes | Treatment Methods |
|---|---|---|
| Elevated | Wound closure under tension | Intralesional corticosteroids |
| Inadequate apposition of wound edges | Shave excision | |
| Full-thickness grafts (commonly oversized) | Fusiform excision | |
| Dermabrasion | ||
| Laser resurfacing | ||
| Hypertrophic | Genetic predisposition | Intralesional corticosteroids |
| scars/keloids | Area of motion or tension | Shave excision |
| Nidus of prolonged inflammation (e.g., infection or | Fusiform excision | |
| foreign body reaction) | Radiation | |
| Cryosurgery | ||
| Lasers | ||
| Compression therapy | ||
| Depressed scar | Deep shave biopsy | Fusiform excision and suture |
| Electrodessication/curettage | with buried vertical mattress | |
| Deficient wound eversion | intradermal sutures | |
| Wound healing complicated by hematoma or infection | Fillers | |
| Subcision/subdermal undermining | ||
| Widened scars | Wounds closed under tension | Excision and suture with buried vertical |
| mattress intradermal sutures | ||
| Long linear scar | Preoperative poor planning | W-plasty |
| Geometric broken line closure | ||
| Dermabrasion | ||
| Pitted/ice pick | Prior acne | Punch excision |
| Trauma | Punch grafting | |
| Dermal pocket grafting | ||
| Dermabrasion | ||
| Contracted/webbed | Traverse concavities | Z-plasties |
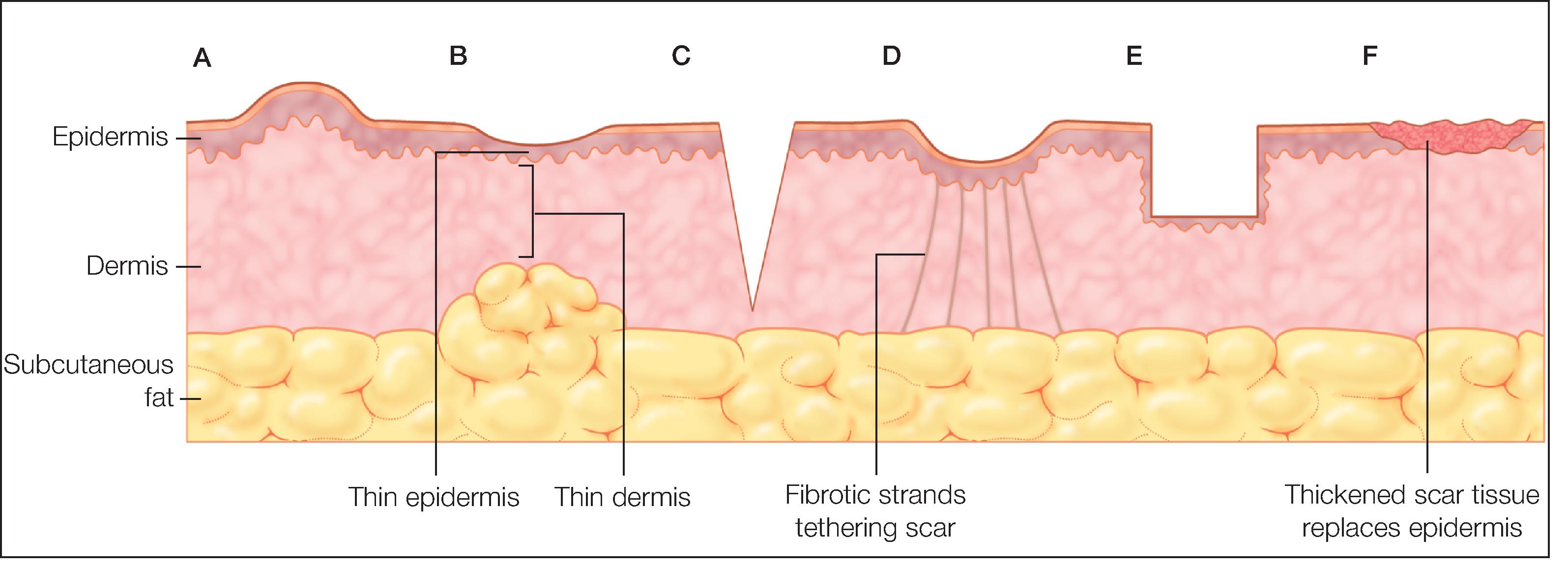
Poorly designed scars generally do not respect one or more of the following: RSTLs, cosmetic unit junctions, facial landmarks, or free tissue margins such as the lip or eyelid. Consequently, they are not well camouflaged and are especially apparent to the observer. The appearance of these scars varies broadly, presenting as elevated, depressed, widened, contracted, webbed, or long and linear. A schematic diagram of different scar types is presented in Fig. 3.2 .
Traumatic scars arise from accidental events such as burns or lacerations and do not have the benefit of careful preoperative planning. Similar to poorly designed scars, these scars do not respect the patient’s anatomy and may present with a variety of clinical features. Furthermore, these scars have unique features based on the type of trauma that caused the scar. Burn scars, for example, may cause severe contraction that leads to an increase in skin tension and a thin atrophic dermis.
Poor healing from infection, excess wound tension, presence of a foreign body, or necrosis with slough can also create disfiguring scars, especially keloidal or hypertrophic scars. A keloid spreads beyond the boundaries of the original wound and is hypertrophic, painful, and pruritic. This scar type develops a median of 30.4 months after injury and can often recur, especially in high-risk sites such as the shoulders, chest, earlobes, upper arms, and cheeks. While the hypertrophic scar also has a raised appearance, its size is limited to the boundary of the original injury and it often occurs in areas of high motion. The hypertrophic scar develops earlier than the keloid, at less than 4 weeks after injury; it is more responsive to intervention, including surgical excision, and more likely to subside with time. Chapter 7 discusses scarring in ethnic populations, including keloidal and hypertrophic scars, in greater depth.
Disease-related scars arising from acute inflammatory processes, such acne vulgaris or varicella zoster, often present as atrophic scars. These scars appear concave and the overlying skin can be paper thin, as the associated inflammation results in collagen destruction with dermal atrophy. Acne scars can be further categorized clinically as ice pick, rolling, and boxcar scars. Ice pick scars are deep punctate scars, while boxcar scars are shallow or deep, flat crateriform depressions in the skin. Rolling scars appear as irregular tethering of the skin, resulting in an uneven superficially wrinkled texture. Ice pick and deep boxcar scars respond well to punch excision, while rolling scars are best treated with subcision, fillers, or lasers. Punch elevation may also be used for wider, deep boxcar scars (>3 mm).
Patient Selection
In theory, any scar with a suboptimal appearance can be revised; however, the greatest patient satisfaction can only be achieved with realistic expectations from both the patient and the dermatologic surgeon. Preoperative consultation should strive to educate and emphasize to the patient that a scar can never be completely removed but only exchanged for a more cosmetically pleasing one. Complete restoration of a scar to its preinjury state is impossible, but careful preoperative planning will significantly reduce the need for future revision.
A number of considerations should be made before attempting a scar revision. A comprehensive patient medical history including response to past surgical procedures should be obtained. Certain patient populations, such as those of Asian, Hispanic, and African descent, are predisposed to developing keloids and hypertrophic scars. Age also plays a factor, as the highest incidence of keloid development occurs between the ages of 10 and 30 years. Further caution should be exercised in patients with genetic disorders, including Ehlers-Danlos and Marfan syndromes; endocrine abnormalities of the hypothalamus, thyroid, and parathyroid glands; or a history of radiation. Any of these conditions may result in an insufficient response to revision and subsequent poor scarring.
Overview of Treatment Strategy
General Treatment Approach
The surgical strategy selected should be based on careful evaluation of the scar’s characteristics: color, texture, type and timing of previous therapy, position and orientation, size, thickness, and quality of the surrounding skin. Special caution should be exercised with “difficult” scars, such as those that result from injuries where skin was lost from avulsion, necrosis, or large excisions, as skin laxity will be significantly diminished. The revision should be planned close to the original scar but not at the edge or margin of the scar.
Preoperative instructions for patients should include the avoidance of anticoagulant medications as medically appropriate including voluntary aspirin, nonsteroidal antiinflammatory drugs, vitamin C and E supplements, and alcohol for at least 1 week. Prophylactic antibiotics against wound infection should also be prescribed when indicated, such as for high-risk surgical sites (e.g., the axilla, perineum, and sites of cartilage exposure) or predisposing medical conditions (e.g., within 2 years after joint or valve replacement or immunosuppression).
General Surgical Principles
Use a marking pen to outline planned incisions with the patient in an upright position prior to infiltration of local anesthetic. Be sure to mark or redefine key anatomic landmarks that may become obscured during surgery (e.g., vermillion border or nasolabial fold).
All procedures described in this chapter are performed under local anesthesia. The authors use 1% lidocaine with 1:100,000 epinephrine for a vasoconstrictive effect in areas with good collateral circulation. The surgical site should undergo sterile prep and drape. A Bard-Parker No. 15 scalpel blade is generally used for excisional surgery.
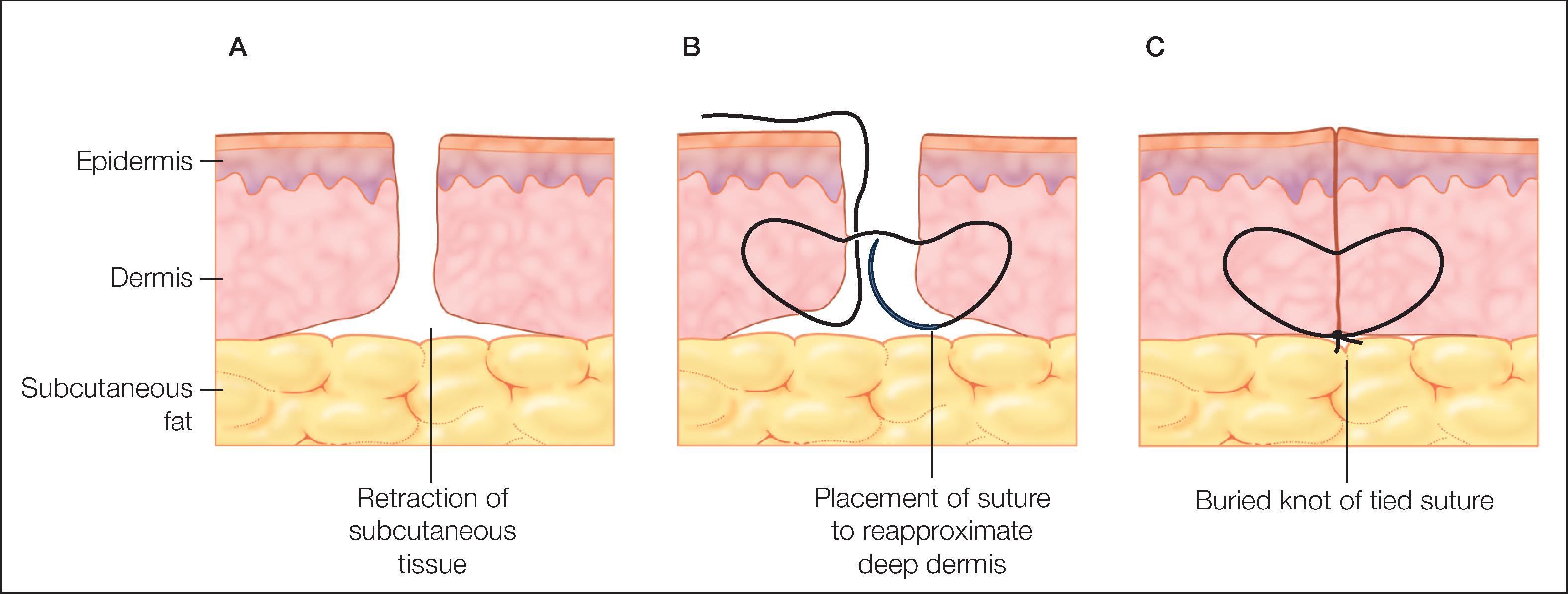
Wounds heal best with clean, fresh, healthy edges; this can be achieved by approximating edges with minimal tension in the correct orientation and with the least reactive suture material selected. The authors employ buried vertical mattress sutures to minimize retraction of the dermis and subcutaneous tissue, which displaces tension off the healing wound edge. A well-placed buried vertical mattress suture as demonstrated in Fig. 3.3 also yields tissue eversion. Suspension or tacking sutures to anchor the advancing tissue edge to periosteum can be employed to decrease tension on a free tissue margin such as the lip or eyelid and to recreate a natural fold or concavity.