The primary goal of cleft palate repair is to create an anatomically and functionally intact palate while minimally affecting maxillary growth and development. In order to produce normal speech, a child must have velopharyngeal competence, defined as the ability to completely close the velopharyngeal sphincter that separates the oropharynx and nasopharynx. The absence of this ability, termed velopharyngeal insufficiency (VPI), is seen in a wide range of patients following primary cleft palate repair. This article discusses patient assessment, treatment options, and the surgical management of VPI. Recent trends and future directions in management are also presented.
Key points
- •
Speech assessment, including nasoendoscopy and multiview video fluoroscopy are essential tools in identifying patients who will benefit from surgical management of velopharyngeal insufficiency and guiding procedure selection.
- •
Although there is no current consensus on the best available technique, many centers select the corrective procedure based on velopharyngeal closure pattern and pharyngeal gap.
- ○
With sagittal closure patterns, double-opposing Z-palatoplasty (DOZ) is effective with small pharyngeal gaps; pharyngeal flaps are used if the gap is large.
- ○
For coronal closure patterns, dynamic sphincter pharyngoplasty (DSP) can be used with small gaps; a combination of DOZ and DSP can be used with large gaps.
- ○
- •
Patients with velocardiofacial syndrome often do well with a high-inset, wide pharyngeal flap procedure. However, alternative surgical techniques are being investigated in these patients.
Overview
The primary goal of cleft palate repair is to create an anatomically and functionally intact palate to improve feeding and achieve normal speech while minimally impacting maxillary growth and development. In order to produce normal speech, a child must have velopharyngeal competence, defined as the ability to completely close the velopharyngeal sphincter that separates the oro- and nasopharynx. The absence of this ability, termed velopharyngeal insufficiency (VPI), is seen in a wide range of patients following primary cleft palate repair, with approximately 20-30% requiring secondary surgical correction.
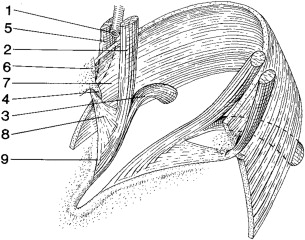
The velopharyngeal mechanism is a muscular valve extending from the posterior bony palate to the posterior pharynx. With the exception of three sounds in the English language (/m/, /n/, /ng/), all speech is produced with a closed velopharyngeal port. The muscles involved in velopharyngeal closure are depicted in Fig. 1 . While understanding the normal anatomy and physiology of this mechanism is essential to appropriate care of the patient with VPI, a full description is beyond the scope of this chapter.
The following will discuss the patient assessment, treatment options, and the surgical management of VPI. Recent trends and future directions in management are also presented. After reading, one should be able to describe the approach to a patient with suspected VPI, including the selection and execution of the appropriate surgical procedure.
Historical perspective
Surgical manipulation of the velopharyngeal port dates back to the nineteenth century. The first recorded attempt by Passavant in 1865 was direct adhesion of the soft palate to the posterior pharyngeal wall. Shoenborn later described the familiar pharyngeal flap operation in 1875, which was popularized in the United States by Padgett in 1930. Subsequent modifications to flap design and orientation have focused on minimizing nasal air emission while preventing airway obstruction. The importance of pharyngeal flap design and orientation continues to be debated in the literature.
In 1950, Wilfred Hynes described an operation to address failed cleft palate repair whereby he secured myomucosal flaps, containing salpingopharyngeus and palatopharyngeus muscles, to the posterior pharyngeal wall. His technique has since undergone several modifications, most notably by Orticochea in 1968, who advocated lower flap inset and inclusion of a third, inferiorly based posterior pharyngeal flap; Jackson and Silverton in 1977, who advocated a combination of palatopharyngeal flaps and a superiorly based pharyngeal flap; and Riski and colleagues in 1984, who advocated higher fixation of the myomucosal flaps to the posterior pharyngeal wall, at or near the point of velar contact. Several additional modifications have been made to each procedure, with various outcomes studies available for each technique.
Augmentation of the posterior pharynx to decrease velopharyngeal port size dates back to the early twentieth century. Beginning with Vaseline in 1900, various materials, including paraffin, cartilage, silicone, porous polyethylene, Proplast, collagen, calcium-hydroxyapatite, Teflon, GoreTex, dermis-fat flaps, and, more recently, autologous fat grafts have all been used to augment the posterior pharyngeal wall. Several of these techniques have shown considerable success in treating velopharyngeal insufficiency (VPI); however, all materials have advantages and disadvantages. With recent advances in autologous fat grafting techniques, there has been increasing focus on the potential for this modality in the treatment of VPI.
Historical perspective
Surgical manipulation of the velopharyngeal port dates back to the nineteenth century. The first recorded attempt by Passavant in 1865 was direct adhesion of the soft palate to the posterior pharyngeal wall. Shoenborn later described the familiar pharyngeal flap operation in 1875, which was popularized in the United States by Padgett in 1930. Subsequent modifications to flap design and orientation have focused on minimizing nasal air emission while preventing airway obstruction. The importance of pharyngeal flap design and orientation continues to be debated in the literature.
In 1950, Wilfred Hynes described an operation to address failed cleft palate repair whereby he secured myomucosal flaps, containing salpingopharyngeus and palatopharyngeus muscles, to the posterior pharyngeal wall. His technique has since undergone several modifications, most notably by Orticochea in 1968, who advocated lower flap inset and inclusion of a third, inferiorly based posterior pharyngeal flap; Jackson and Silverton in 1977, who advocated a combination of palatopharyngeal flaps and a superiorly based pharyngeal flap; and Riski and colleagues in 1984, who advocated higher fixation of the myomucosal flaps to the posterior pharyngeal wall, at or near the point of velar contact. Several additional modifications have been made to each procedure, with various outcomes studies available for each technique.
Augmentation of the posterior pharynx to decrease velopharyngeal port size dates back to the early twentieth century. Beginning with Vaseline in 1900, various materials, including paraffin, cartilage, silicone, porous polyethylene, Proplast, collagen, calcium-hydroxyapatite, Teflon, GoreTex, dermis-fat flaps, and, more recently, autologous fat grafts have all been used to augment the posterior pharyngeal wall. Several of these techniques have shown considerable success in treating velopharyngeal insufficiency (VPI); however, all materials have advantages and disadvantages. With recent advances in autologous fat grafting techniques, there has been increasing focus on the potential for this modality in the treatment of VPI.
Patient assessment
Patient History
As with all surgical patients, the assessment of a patient presenting with evidence of VPI should begin with a thorough history and physical examination. In particular, the onset of speech anomalies, previous history of cleft lip and/or cleft palate (CLP), as well as any previous palatopharyngeal surgery (tonsillectomy, adenoidectomy, and so forth) or neurologic disorders should be elucidated.
A history of repaired or unrepaired cleft palate is the most common cause of VPI. The most common causes of VPI in children with a history of repaired cleft palate are inadequate lengthening of the velum at the time of primary palatoplasty, abnormal function of the levator musculature, and cicatricial contracture of the velum. Other causes include submucous cleft palate; neurogenic VPI caused by central or peripheral insults to the cranial nerves innervating the velopharyngeal mechanism; and iatrogenic VPI following maxillary resection, uvulopalatopharyngoplasty, or adenoidectomy. Although physiologic involution of the adenoid pads can result in VPI, these structures are not thought to function in normal velopharyngeal closure. Patients with progressive pubertal VPI in the absence of adenoidectomy are rare and are thought to have underlying velopharyngeal disproportion. The causes of structural, functional, and dynamic VPI are summarized in Table 1 . For a more comprehensive discussion of the multiple causes of VPI, including their diagnosis and management, readers are directed to several excellent review articles.
| Diagnosis | ||
|---|---|---|
| Mechanism | Congenital | Acquired |
| Structural Abnormalities | ||
| Palatopharyngeal disproportion |
|
|
| Abnormal anatomy of levator palati muscles |
| |
| Functional Abnormalities | ||
|
| |
| ||
| Palatal Paresis | ||
| Upper motor neuron |
|
|
| Nuclear |
|
|
| Peripheral nerve | — |
|
| Myoneural junction | — |
|
| Primary muscular abnormality |
|
|
| Nonspecific or undetermined cause |
| — |
| Obstructive and Restrictive Causes |
|
|
Speech Assessment
A detailed discussion on speech assessment is provided by Kummer and colleagues elsewhere in this issue.
It is of paramount importance for the child with suspected VPI to undergo formal evaluation by a speech-language pathologist before considering surgical intervention. This evaluation begins with a perceptual speech evaluation to assess articulation, resonance, nasal airway emission, and voice.
Multiple scales exist for evaluation of velopharyngeal function. In our practice, we use the Pittsburgh Weighted Speech Score (PWSS) to grade VPI on a quantitative scale. This scale uses a standardized scoring system to evaluate a patient based on nasal air emission, facial grimace, resonance, voice quality, and articulation. A sample patient assessment worksheet is shown in Fig. 2 . The individual scores are summed, and the total scores are used to classify patients into one of 4 categories of velopharyngeal function (in increasing order of dysfunction): competence, borderline competence, borderline incompetence, and incompetence.
If the formal speech evaluation indicates borderline or frank velopharyngeal incompetence (PWSS score of 3 or greater), adjunctive studies are available to guide the selection of the best intervention.
Instrumental Assessment of the Velopharyngeal Mechanism
There are several diagnostic modalities available to image the dynamic function of the velopharyngeal mechanism and determine its pattern of closure. The 3 basic closure patterns are described as:
- 1.
Coronal, in which movement of the velum is primarily responsible for velopharyngeal closure, with little contribution from the lateral pharyngeal walls
- 2.
Sagittal, in which medial displacement of the lateral pharyngeal walls is primarily responsible for closure, with little posterior movement of the velum
- 3.
Circular, in which movement of the velum and the pharyngeal walls contribute to a sphincteric or purse-string closure of the velopharyngeal port
The most common diagnostic evaluations of velopharyngeal function and closure pattern are nasoendoscopy and multiview video fluoroscopy. Nasoendoscopy uses a flexible endoscope inserted through the middle meatus to the posterior pharynx to visualize the velopharyngeal mechanism from a bird’s-eye view while the patient phonates a speech sample. Nasoendoscopy provides visualization of the size and location of the velopharyngeal opening and relative contributions of the velum, lateral pharyngeal walls, and posterior pharynx during attempted velopharyngeal closure. Nasoendoscopy is also useful to assess for palatal scarring, oronasal fistulae, submucous clefting, and the status of the tonsils and adenoids.
Multiview video fluoroscopy (MVF) involves imaging of the same speech sample through multiple views, including lateral and anterior-posterior views to evaluate the relative contributions of the velum and lateral pharyngeal walls in attempted closure, respectively. Although MVF can be useful in identifying the point of attempted velar contact, it is limited in its ability to measure multiple variables in a single view. Therefore, most clinicians prefer to use MVF in conjunction with nasoendoscopy. MVF is also useful with children who do not tolerate nasoendoscopy. Although these modalities provide complementary information in assessing the velopharyngeal closure pattern, nasoendoscopy has been shown to correlate more strongly with VPI severity.
Magnetic resonance imaging (MRI) has gained popularity in recent years as an imaging modality that may provide better-tolerated and more precise information regarding the anatomy of the velopharyngeal mechanism. Clear benefits of this technology include its noninvasive nature and avoidance of ionizing radiation in a mostly pediatric population. Although several centers have reported success with this technique, limitations remain in its ability to obtain clear images with short enough exposure time to limit motion-related artifact during dynamic speech. With the further development and refinement of MRI technology, this may offer a more precise and better-tolerated assessment of the velopharyngeal mechanism during speech.
Nasometry is a technique that can provide objective measurement of the acoustic energy emitted from the nasal cavity relative to that of the combined oral and nasal cavities. To achieve this, the nasometer consists of a headset with 2 microphones positioned in front of the nose and mouth with an intervening metallic plate to isolate acoustic energy from each cavity. The headset is connected to a computer that interprets and graphically represents the proportion of nasal/total acoustic energy emission as nasalance scores (0–100) for comparison with available normative data. Although this modality provides a purely objective assessment of acoustic energy distribution, it is best used as an adjunctive measure to perceptual speech assessment to provide the most comprehensive speech assessment.
Current practice
Available treatment options for VPI include speech therapy, prosthetic devices, and surgical management. Although prosthetic devices are usually reserved for patients who are considered poor surgical candidates, or for whom surgical treatment is not available, they have shown a high success rate in the treatment of VPI. The most commonly used techniques for the surgical management of VPI are:
- 1.
Furlow palatoplasty, or double-opposing Z-plasty, for palatal lengthening
- 2.
Pharyngeal flap
- 3.
Dynamic sphincter pharyngoplasty (DSP)
Although some investigators have also advocated the use of posterior pharyngeal augmentation, by means of injectable or implantable alloplastic and autologous materials, these techniques are not currently in widespread use and are not discussed in detail in this article. The reader is directed to the references provided for additional information regarding these modalities.
Authors’ preferred technique
Preoperative Planning
A detailed knowledge of the patient’s history and mechanics of attempted velopharyngeal closure usually suffice in determining the best course of surgical treatment. As mentioned previously, closure of the velopharyngeal mechanism depends primarily on the elevation and posterior motion of the velum; however, important contributions are made by movement of the lateral pharyngeal walls toward the midline as well as anterior bulging of the posterior pharyngeal wall. The success of surgical correction of VPI depends as much or more on the selection of the appropriate procedure than on technical expertise. In our experience, a perfectly performed procedure cannot correct VPI in an improperly selected patient and may increase upper airway complications. To that end, any surgical procedure performed to address VPI should take into consideration the existing pattern of velopharyngeal closure.
Algorithmic Approach to Procedure Selection
Our surgical approach is selected based on the pattern of velopharyngeal closure and the pharyngeal gap, or size of the aperture present with attempted closure. For patients with a sagittal pattern of closure, the deficiency lies in a lack of posterior velar movement or in palatal length; therefore, for patients with this closure pattern and a pharyngeal gap of less than 9 mm, palatal lengthening alone is often sufficient, and we prefer using a double-opposing Z-palatoplasty (DOZ). In patients with a sagittal closure pattern and a gap of greater than 9 mm, a superiorly based pharyngeal flap is a good solution. The airway concerns commonly associated with pharyngeal flaps are less likely to occur in these patients because the lateral pharyngeal wall mobility allows opening of the lateral velopharyngeal ports.
In patients with poor lateral wall motion (coronal closure pattern), the velum is the primary contributor to velopharyngeal closure. In such patients, with a velopharyngeal gap of 9 mm or less, DSP is preferred rather than a pharyngeal flap. In these patients, the poor motion of the lateral walls may contribute to nasal airway obstruction should a pharyngeal flap be attempted.
Patients who have a coronal closure pattern with a pharyngeal gap of more than 9 mm present a challenging problem. Based on a review of 13 patients with such velopharyngeal mechanics, we have found that the combination of DOZ and DSP works well to lengthen the palate, which, combined with the sphincteric motion of the DSP, can effect velopharyngeal competence. In this series, 15% of patients had persistent hypernasality, which was corrected in all cases with secondary placement of a narrow pharyngeal flap. The combination of DOZ and DSP was shown to significantly improve speech and voice ratings on a standardized scale.
For patients with a circular, or sphincteric, closure pattern, but persistent pharyngeal gap, the procedure of choice depends on the gap size. If there is a small gap (<9 mm), our procedure of choice is the DOZ; for large gaps, narrow pharyngeal flaps are used, because the adequate lateral wall motion allows closure of the lateral ports and minimizes risk of airway obstruction.
In general, our preference is to use a pharyngeal flap as a last resort, except in cases of velocardiofacial syndrome (VCFS), as described later.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


