CHAPTER 31 Superomedial Pedicle Extension Mastopexy
Key Points
Summary
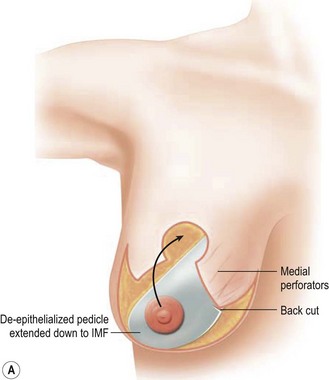
Superomedial pedicle extension flaps essentially involve the rotation of lower pole dermatoglandular tissue attached to the superomedial nipple–areola complex (NAC) pedicle and moved to remote areas in the breast where additional volume is required (Fig. 31.1). All breast reduction and mastopexy techniques rely on repositioning the NAC on a vascularized pedicle, resecting tissue as needed, and reshaping the breast mound with the pedicle and residual breast tissue. Extension flaps and autoaugmentation techniques are relatively new and are slightly more involved. In addition to relying on residual breast tissue for shape and size, they rotate local or distant flaps from one region of the body to fill an area of volume void within the breast. Although distant flaps have been reported, the majority of autoaugmentation techniques are local from the thoracic or abdominal region, or from within the breast. Local ‘non-breast’ options for autoaugmentation techniques typically use fasciocutaneous flaps or perforator flaps from the lateral chest wall or upper abdominal region.1–4 Local breast flaps are dermatoglandular flaps or glandular flaps based off the chest wall or as extension flaps from various NAC pedicles.5–7 Although these autoaugmentation techniques were initially used to improve shape and volume in mastopexy cases, they have become more popular recently out of necessity in the management of the massive weight loss breast, and partial mastectomy defects.

Patient Selection
Numerous options exist for extending pedicles to autoaugment certain locations within the breast. Surgeons will often rely on a technique that they are familiar with and modify their approach to best address the deformity. Various authors have employed central or inferior pedicle techniques, and designed vascularized attachments to provide suspension of the breast mound, and autoaugmentation mainly in the upper pole where volume is often desired.6,7 Although the majority of surgeons still use the inferior pedicle breast reduction technique,8 there is a growing trend toward the more superiorly based pedicle designs. It is felt that the superomedial pedicle technique can afford more reliable cosmetic outcomes, shorter operating times, and less pseudoptosis.9,10 The superomedial pedicle is a relatively short, well-vascularized pedicle that can easily rotate into position.
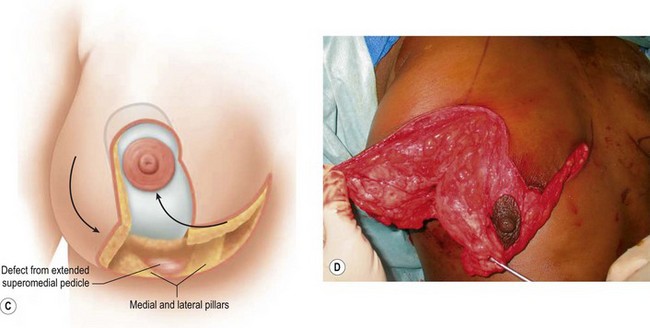
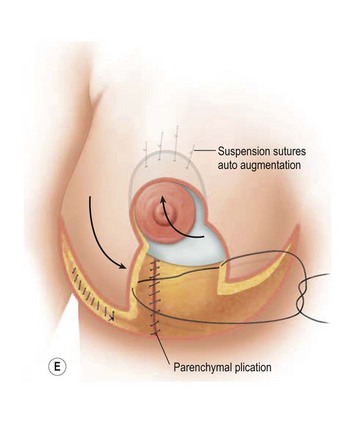
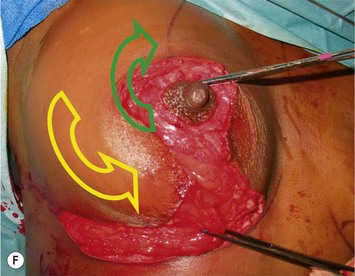
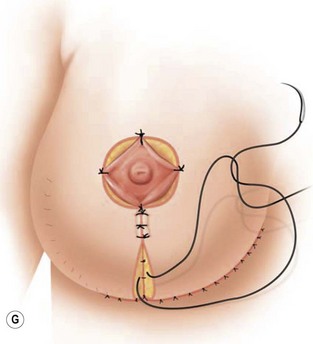
Breast reduction techniques using superiorly based pedicles, whether superior or superomedial, both have the excess dermatoglandular tissue resected in an ‘en bloc’ wedge type fashion from the lower pole. This tissue is subsequently very amenable to being used as a vascularized extension of the NAC pedicle design for rotation to fill the upper or outer breast quadrant. Graf initially described the use of this lower pole breast tissue as a weaving technique through the pectoralis muscles to autoaugment the breast mound in mastopexy techniques.11 Although it can also be used as an extended superior pedicle flap, this chapter is going to focus on it being rotated as an extended superomedial pedicle. Many of the advantages of the superomedial technique as described by Hall-Findlay can also be applied to the extended superomedial technique.10,12 The extended pedicle is easily rotated laterally and superiorly with the NAC to provide elevation of the nipple and autoaugmentation of the upper or lateral breast. This is a more natural arc of rotation than the extended superior pedicle where the nipple needs to move superiorly, and the pedicle extends below the nipple and is then tucked superiorly. Dermal release below the nipple is often required when using the extended superior pedicle, which could potentially compromise viability of the extension. The extended superomedial pedicle takes tissue from the lower pole where volume is often less desirable, and rotating it to the upper pole where there is often a volume void. This also leaves a lower pole defect, amenable to parenchymal plication with the added benefits of glandular reshaping, narrowing the breast mounds, tightening the IMF and minimizing recurrent ptosis (Fig. 31.1). This extended superomedial technique can be used with a vertical or a standard Wise mastopexy skin pattern.
Indications
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


