Supermicrosurgery is defined as microsurgery working on vessels less than 0.8 mm, allowing applications in smaller-dimension microsurgery, such as lymphedema, minimal invasive reconstruction, small parts replantation, and application of perforator as recipient. To accommodate this technique, developments and use of finer instruments, smaller sutures, new diagnostic tools, and higher-magnification microscopes have been made. Although supermicrosurgery has evolved naturally from microsurgery, it has developed into a unique field based on different thinking and tools to solve problems that once were difficult to solve.
Key points
- •
Supermicrosurgery is defined as manipulation of vessels less than 0.8 mm, often requiring different thinking and tools.
- •
Perforators can be used as a recipient source (perforator-to-perforator supermicrosurgery), minimizing the need for extensive dissection to find recipient vessels.
- •
Perforators also allow reconstruction, where axial arteries are not available due to trauma, atherosclerosis, or other causes.
- •
Like a perforator flap based on a single perforator, the limits of a single perforator as a recipient should be understood.
Introduction
Microsurgery is a general term for surgery requiring the use of an operating microscope; in the field of reconstructive surgery, various procedures are performed, such as replantation, flap transfer, autotransplantation or allotransplantation, revascularization, neurorrhaphy, lymphatic surgery, and others. The core principles of microsurgery encompass (1) proper working environment, including microscopes and loupes; (2) preoperative evaluation and planning; (3) microsurgical technique from elevation, pedicle dissection, recipient preparation, microanastomosis, to flap insetting; and (4) postoperative care. The reconstructive microsurgery usually involves the anastomosis of vessels of approximately 1 mm to 2 mm in vessel diameter. In some instances of larger vessels, anastomosis can be done under loupe magnification. The overall success rates for reconstructive microsurgery in the lower extremity using these principles are approximately 93% to 100%. Although lower extremity reconstructive microsurgery remains the highest rung of the reconstruction ladder, the goal of microsurgery is stretched to achieve not only soft tissue coverage but also function and acceptable aesthetics through a more efficient reconstructive elevator approach, simplifying the stages of reconstruction.
The wide zone of injury, however, usually associated with trauma frequently leaves the extremity with injured vessels; the increase in chronic diseases among the general population leaves the axial arteries calcified; the axial arteries often are difficult to approach, especially when reconstructing the upper leg including the knee; and, when using a single axial artery, there is a fear of steal phenomenon, making lower extremity reconstruction challenging. These situations frequently result in limited availability of good pulsatile axial arteries as choices for recipient vessels. Even when using these limited axial arteries as recipient sources, the possibilities of having steal phenomenon and injuring the functioning artery may deter surgeons from using these axial arteries. Thus, utilizing the recipient from the contralateral leg spared from injury in a cross-leg fashion can be a reliable source. Although this approach deserves to be recognized and should be considered an alternative solution, the process is painstaking not only for surgeons but also for patients. Knowing that the first key to having a successful outcome for microsurgical reconstruction is having a reliable recipient source, it must be asked how to overcome these difficulties in finding a reliable recipient.
In the era of perforator flaps, which are cutaneous or fasciocutaneous flaps based on a single perforator, it is remarkable to see a flap with a large skin dimension have a successful outcome reflecting the influence of a single perforator. The authors hypothesized that if a single perforator is capable of supplying the skin vascularity, it could be used as a recipient source. , In the past, it was believed that there was a significant risk for failure in using vessels with diameter less than 1 mm. Since the early days of microsurgery, there has been substantial improvement of microscopes, technique, instruments, training, knowledge, and imaging, allowing microsurgeons to perform anastomosis of vessels less than 1 mm without worrying about the outcome. Hence, the term, supermicrosurgery technique , is defined as microsurgical anastomosis of vessels with a diameter less than 0.8 mm facilitated by using smaller and finer instruments. , This technique frequently is applied to lymphaticovenous anastomosis (LVA) to treat lymphedema, fingertip replantation, finger/toe reconstruction, and nerve flaps and in soft tissue reconstruction. The use of a perforator as a recipient vessel in the lower extremity falls into this domain because a majority of the perforators used are less than 0.8 mm, and numerous articles have validated the efficacy of the approach. , , In this article, principles, indications, preoperative evaluation, surgical procedures, postoperative care, and management of complications after perforator-to-perforator supermicrosurgery are presented and reviewed.
Indications and contraindications
Any perforators that are pulsating can be indicated for use as a recipient source. These perforators can be found within the defect while débriding or adjacent to this zone. Unlike burns and radiation wounds, the zone of injury, especially in trauma, is difficult to define and the definition remains unclear. Nevertheless, the zone of injury concept should be considered and using a vessel within the zone avoided if a good alternative exits nearby, because perivascular changes within the zone may occur and lead to increased friability of vessels and perivascular scarring of recipient vessels, resulting in higher incidence of thrombosis after anastomosis. If choosing to use a recipient vessel within the zone, clinical presentation of vessel wall pliability and quality of blood from transected vessel need to be feasible to have a successful outcome. This idea was validated further by using a perforator as a recipient adjacent to or within zone of injury. When large vessels are readily available or superficially located, however, then these vessels should be chosen as it will be technically easier. In cases of large axial vessels anatomically located deep to the muscles, injured or calcified, patients benefit the most from using a perforator as a recipient.
A large perforator with adequate flow is able to supply a large territory of skin. When using a perforator as a recipient, the limit of perfusion from the perforator needs to be understood. It would not be feasible to use a perforator to supply a large muscle or a chimeric flap that requires abundance of flow. Thus, an adequate indication to use the perforator as a recipient vessel would be a skin or fasciocutaneous flap that is sufficiently supplied by vascularized by 1, 2, or 3 angiosomes. Although multiple variables may determine the success of the flap after perforator-to-perforator approach, a simple and safe way to determine the adequacy of flap size is to see the viability of the flap during the elevation before cutting the pedicle based on a single perforator.
Preoperative evaluation and special considerations
When microsurgical reconstruction is planned, evaluating the vascular status of the lower extremity is essential not only to understand the vasculature of the major axial arteries but also to identify potential recipient arteries as well as potential donor sites. The use of preoperative arteriography for lower extremity reconstruction is considered when physical/Doppler examination reveals inconclusive vascular status or chronic vascular disease is suspected. According to the authors’ experience, 75% to 80% of lower extremity reconstructions that involve trauma, chronic wounds, and oncologic reconstruction undergo detailed vascular evaluation. The computed tomographic angiography (CTA) is minimally invasive and can be obtained easily, revealing adequate information facilitating the planning and the surgical procedure. , The invasive angiogram is reserved for patients who need intervention to revascularize the extremity or if the presence of foreign bodies makes CTA difficult to read. From both modalities, when looking at defect region, perforators often are identifiable, allowing consideration as a recipient vessel. Then, using a handheld Doppler, the location of the target perforator can be pinpointed. The use of duplex ultrasound, however, is becoming the main modality in identifying perforators. It has multiple advantages over CTA and handheld Doppler. It is able not only to provide real-time reading of the exact anatomic location and pathway in respect to the skin surface but also to provide physiologic information, such as flow velocity and volume. Perforator velocity greater than 15 cm/s to 20 cm/s as a recipient in ischemic diabetic foot reconstruction is shown to be reliable with acceptable success. Despite the use of these preoperative diagnostics, the key remains to be identifying a good pulsatile perforator during the operation.
Surgical procedure
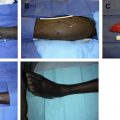
While excising or débriding, perforators that are pulsating within the zone of injury/defect may be seen and may be selected for use as recipient. Working in the zone of injury/defect, however, can be difficult and tedious. Thus, moving away from this zone and based on the prior markings for potential recipient perforators can make the process for locating recipient perforators easier. When exploring for the perforators, they can be found in the same manner as elevating the flap above the fascia if located under the skin or can be searched subfascially depending on surgeon preference. , Initially, the recipient perforators are searched under loupe magnification and, upon location, further dissection is carried out under microscope. If the target perforator is within the zone of defect, dissection is recommended under the microscope to minimize injury to the vessel, which can be surrounded by scarring. A strong visible pulse of the perforator is the main indicator for use. , , When the perforator diameter is too small or with spasm, then dissection can proceed more proximal to the source vessel, which has larger diameter and is less sensitive to manipulation. Fig. 1 shows the approach to securing the recipient perforator. After determining the perforator feasible to use as a recipient vessel, the required pedicle length of the flap is measured. Also, definitive débridement is performed, preparing the recipient site ready for flap coverage. The flap for coverage then is elevated with a corresponding pedicle length and dimension of skin for coverage. Usually, a short pedicle suffices, saving operating time for pedicle dissection. Swelling must be anticipated, however, and it must be ensured that swelling does not increase tension to the anastomosis site and thus harvest an extra centimeter or 2. Prior to transecting the pedicle from the donor site, status of the recipient perforator is checked again. A strong pulse or a pulsatile flow after opening the vessels is the indicator to proceed for anastomosis. This allows the surgeon to fix the problem before it becomes a major problem.

Related posts:
 Propeller Flaps in Lower Extremity Reconstruction
Propeller Flaps in Lower Extremity Reconstruction
 The Medial Sural Artery Perforator Flap in Lower Extremity Reconstruction
The Medial Sural Artery Perforator Flap in Lower Extremity Reconstruction
 Free-Style Free Perforator Flaps in Lower Extremity Reconstruction
Free-Style Free Perforator Flaps in Lower Extremity Reconstruction
 Orthoplastic Approach to Lower Extremity Reconstruction
Orthoplastic Approach to Lower Extremity Reconstruction
 The Anterolateral Thigh Perforator Flap
The Anterolateral Thigh Perforator Flap
 Lower Extremity Reconstruction in the Pediatric Population
Lower Extremity Reconstruction in the Pediatric Population
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


