Superior Gluteal Artery Perforator Flap Breast Reconstruction
Katie E. Weichman
DEFINITION
The superior gluteal artery perforator (SGAP) flap is a variation of the gluteal artery myocutaneous flap initially described by Shaw and further modified by Codner and Nahai for use in breast reconstruction.1,2 This perforator flap was first described as a pedicled flap by Koshima and used for repair of sacral pressure sores3 and further expanded for use as a free flap in breast reconstruction when described by Allen and Tucker in 1995.4 This perforator flap uses skin and tissue in the buttock area based on the SGAPs. The flap has been further modified by Blondeel in 1999 for use in breast reconstruction as a sensate flap.5
While abdominally based free flaps remain the most common choice for breast reconstruction secondary to sufficient skin and soft tissue, patients may require alternative donor sites for various reasons. These reasons include lack of abdominal donor sites secondary to prior abdominoplasty, inadequate volume in the abdomen, and patient preference.
ANATOMY
The superior gluteal artery originates from the internal iliac artery and is its largest branch. It runs backward between the lumbosacral trunk and the first sacral nerve and exits the pelvis through the sciatic foramen just above the upper border of the piriformis muscle and inferior to the gluteus medius.
Anatomically, this exit point between the piriformis and the gluteus medius has been shown to be about 6 cm from the PSIS and 4.5 cm lateral to the midline of the sacrum or at the junction of the proximal and middle thirds of a line connecting the PSIS to the apex of the greater trochanter of the femur (FIG 1).
Once it passes out of the pelvis, it immediately divides into a superficial and deep branch.
The superficial branch enters the deep surface of the gluteus maximus muscle and divides into several branches that perforate through the gluteus maximus muscle onto the skin. These are the perforating vessels that will be followed in SGAP dissection.
The superior gluteal vein is associated with the superior gluteal artery; however, it receives multiple tributaries as it enters the pelvis that requires ligation during harvest.
The perforating vessels are located inferior to and lateral to the anatomical exit point of the superior gluteal artery. Several studies have looked at these perforating vessels and found SGAP flaps have a mean number of 7.2 perforators (range 5-10), with an average intramuscular length of 5.33 cm (range 3-11 cm) and a mean total pedicle length of 9.8 cm (range 6.0-15.5 cm).6
There are several muscles that are highlighted for SGAP dissection in the posterior gluteal area (FIG 2).
Gluteus maximus
Origin: Gluteal surface of the ilium, lumbar fascia, sacrum, and sacrotuberous ligament
Insertion: Gluteal tuberosity of the femur and iliotibial tract
Action: External rotation and extension of the hip joint
Arterial supply: Superior and inferior gluteal arteries
Innervation: Inferior gluteal nerve (L5, S1, and S2)
Gluteus medius (deep to the gluteus maximus)
Origin: Gluteal surface of the ilium
Insertion: Greater trochanter of the femur forming the iliotibial tract
Action: Abduction of the hip, preventing adduction of the hip, and medial rotation of the thigh
Piriformis (deep to the gluteus maximus)
Origin: Anterior portion of the sacrum
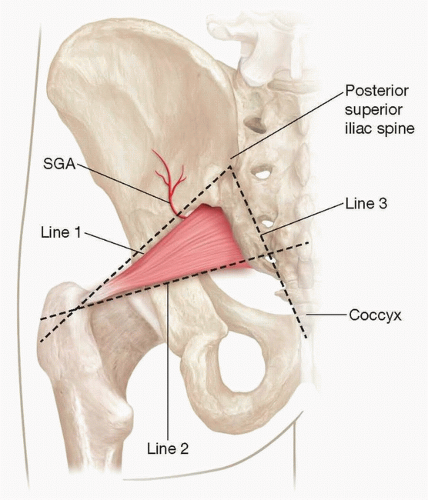
FIG 1 • Anatomical relationships of superior gluteal artery. Line 1 connects posterior iliac spine to apex of greater trochanter. Superior gluteal artery is located at the junction between the proximal and middle third of this line. Line 2 connects the midpoint of the gluteal crease to the superior greater trochanter. Line 3 connects the posterior iliac spine to the coccyx. Line 2 represents the inferior border of the piriformis muscle.
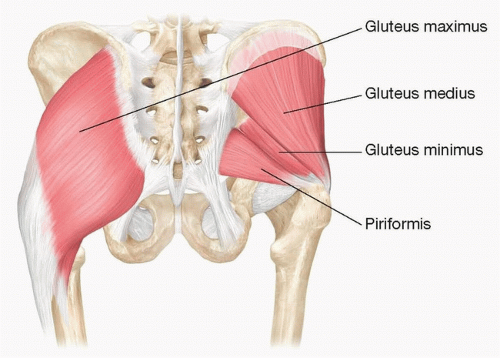
FIG 2 • Important musculature of the posterior trunk involved in SGAP dissection.
Insertion: Greater trochanter of the femur forming the iliotibial tract
Action: External rotator of the thigh
Arterial supply: Interior gluteal artery, superior gluteal artery, and lateral sacral artery
Innervation: Nerve to the piriformis (L5, S1, and S2)
Gluteus minimus (deep to gluteus maximus and gluteus medius)
Origin: Ilium under the gluteus minimus
Insertion: Greater trochanter of the femur forming the iliotibial tract
Action: Works in concert with gluteus medius: abduction of the hip, preventing adduction of the hip, and medial rotation of the thigh
Arterial supply: Superior gluteal artery
Innervation: Superior gluteal nerve (L4, L5, S1)
PATIENT HISTORY AND PHYSICAL FINDINGS
This includes patients with a history of breast cancer, patients undergoing prophylactic mastectomy, patients with congenital abnormalities, and transgender patients.
Physical examination includes examination of the abdomen, medial thighs, and buttock to assess availability of excess tissue.
Timing of reconstruction should be planned in patients with prior history of breast irradiation. The authors prefer to wait 6 months after the completion of radiation therapy prior to completing delayed reconstruction.
Smoking status is also assessed.
Additionally, tamoxifen should be held 3 weeks prior to surgery.
IMAGING
Patients considering SGAP flap reconstruction should undergo preoperative imaging with either computed tomography angiogram (CTA) or magnetic resonance angiography (MRA) of the pelvis and lower extremity.
Imaging is performed in the prone position and coordinating with the radiologist for appropriate evaluation of images.
Perforators should be described as they exit the deep muscular fascia and described based on location in an x–y axis. The gluteal fold will be set as zero on the y-axis, and the midline will be set as zero on the x-axis. Important bony landmarks that should be noted include the coccyx, the summit of the posterosuperior iliac crest, and the most lateral point of the greater trochanter7 (FIG 3).
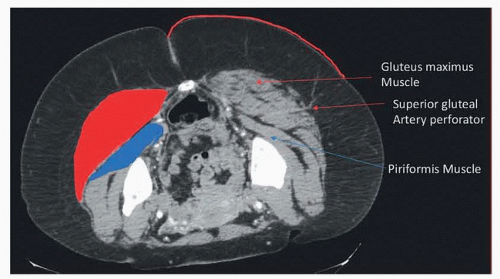
FIG 3 • Locations of SGAP perforator on axial CT scan including the gluteus maximus muscle and piriformis muscle.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree

 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access






