Superior Gluteal Artery Perforator Flap
Lauren M. Mioton
Gregory A. Dumanian
DEFINITION
The superior gluteal artery flap is relevant to the treatment of pressure ulcers, coverage of the lower lumbar spine, and breast reconstruction.
ANATOMY
The superior gluteal artery is a continuation of the posterior division of the internal iliac artery (FIG 1).
It runs between the lumbosacral trunk and the first sacral nerve.
It exits the pelvis above the piriformis and immediately divides into superficial and deep branches.
The deep branch passes between the gluteus medius and the iliac bone.
The superficial branch continues on to supply the upper portion of the gluteus muscle and overlying fat and skin.
The superior gluteal nerve supplies this flap.
It arises from the dorsal divisions of the 4th and 5th lumbar and 1st sacral nerves.
It exits the pelvis through the greater sciatic foramen with the superior gluteal vessels.
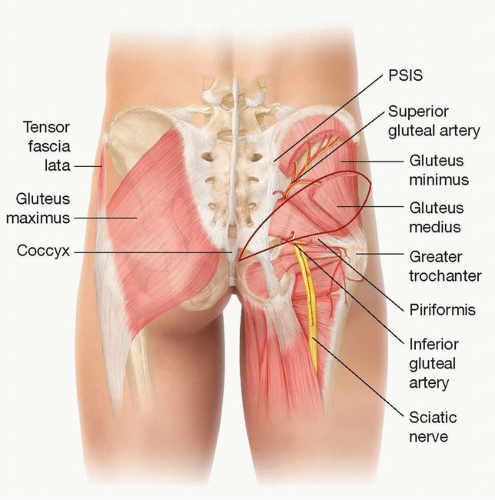 FIG 1 • Anatomic landmarks of piriformis, superior gluteal artery, and superior cluneal nerve. |
PATIENT HISTORY AND PHYSICAL FINDINGS
A thorough history and physical examination should be performed on the patient in the preoperative setting.
Prior lower surgery in the gluteal region should be noted as it may preclude the use of the SGAP flap. A history of spina bifida could be associated with lack of formation, small size, or aberrant location of the superior gluteal artery.
IMAGING
Specific preoperative imaging is not standard workup for SGAP flaps, though it could be performed with a computed tomography angiography.
SURGICAL MANAGEMENT
The SGAP flap can be used for pressure ulcer reconstruction. Additionally, it is a dependable option for autologous breast reconstruction when abdominal tissue is not available.
When designing the SGAP flap, the incisions can be in an oblique or more horizontal orientation. A horizontal scar is often deemed more cosmetically acceptable.
Beveling on dissection creates more dead space and can therefore lead to greater seroma development. Positioning the SGAP more superiorly on the buttock allows for beveling more superiorly and is often associated with decreased revision rates and contour deformities.
Perforators designed more laterally will lead to longer pedicles.
The average height and length of the SGAP flap are 10 and 24 cm.
Preoperative Planning
Patients should undergo additional medical clearance pending their comorbidities.
The SGAP flap should be avoided in severely obese patients.
Positioning
Positioning for an SGAP flap depends on the area to be reconstructed.
For pressure sore reconstruction or bilateral breast reconstruction, the patient should be placed in the prone position with the arms tucked.
In the cases that an SGAP flap is being used for unilateral breast reconstruction, the patient may be in the lateral decubitus position.
In both bilateral and unilateral breast reconstruction cases, the patient is subsequently rolled supine for final flap inset. They should be re-prepped and draped during the position change.
Approach
Markings are placed on the patients in the position that they will be in the OR.
A line is drawn from the posterosuperior iliac spine (PSIS) to the superior portion of the greater trochanter of the femur. The superior gluteal artery exits the greater sciatic foramen and enters the buttock at the junction of the proximal and middle thirds of this line. The location is confirmed with a handheld Doppler probe.
Another line is drawn from the PSIS to the coccyx. The intersection of this line with the superior edge of the greater trochanter helps identify the position of the piriformis.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree