In dorsal preservation rhinoplasty, resection of the septum is required to remove a hump. Modifications to the original immediate subdorsal strip excision of Goodale and Lothrop include the following sub-dorsal approaches: modified subdorsal strip method, Z-flap, intermediate septal strip, and Tetris concept. All of these subdorsal flap techniques are similar in using carefully designed septal cuts to excise and/or mobilize a dorsal cartilaginous segment for dorsal flexion and lowering. The growing body of outcomes data suggests satisfactory results and limitations of each of these septal approaches.
Key points
- •
Subdorsal septal flaps used in dorsal preservation rhinoplasty include the intermediate septal strip, modified subdorsal strip method, Z-flap, and the Tetris concept.
- •
Subdorsal flap techniques are similar in using carefully designed septal cuts to excise and/or mobilize a dorsal cartilaginous segment for dorsal flexion and lowering.
- •
Existing outcomes data suggests satisfactory results from each subdorsal septal flap technique, although comparative data are limited.
Introduction
Dorsal preservation rhinoplasty (DPR) techniques date back to the 19th century with work by otolaryngologists Joseph Lincoln Goodale and Oliver Ames Lothrop, parallel to hump resection techniques described by J. Joseph. However, DPR has grown in popularity among rhinoplasty surgeons in the last 5 to 6 years. , Fundamentals to dorsal preservation ideology are medial keystone preservation and osseocartilaginous continuity. The process requires both 1. disarticulation of the external bony vault from adjacent attachments and 2. resection and mobilization of the septum. Regarding septal resection, a high subdorsal strip resection was originally described and is utilized by many. This has undergone evolution with a variety of modified approaches to the septum, typically classified by the location of septal cartilage excision: subdorsal, mid-septal, or inferior septal (also termed high, intermediate, and low excision technique) ( Fig. 1 ). The purpose of this work is to review and highlight the existing descriptions and evidence for various septal approaches employed in DPR, with particular attention to subdorsal flaps.
Discussion
Septal Anatomy in Dorsal Preservation Rhinoplasty
A review of the anatomy of the septum and its relationship with surrounding nasal structures facilitates understanding of the mechanisms and potential benefits of various septal approaches in DPR. The septum is composed of bony (perpendicular plate of the ethmoid bone and vomer) and cartilaginous (quadrangular cartilage) portions. The cartilaginous portion of the septum does not terminate at the level of the rhinion (the dorsal bony-cartilaginous junction); instead, it extends posteriorly underneath the nasal bones. This most cranial cartilaginous-bony junction has been coined the Ethmoidal (E), Keystone (K), or Junctional (J) point. The distance from the rhinion to the ethmoidal point varies, and distances of 4 to 11 mm have been reported. Therefore, a dorsal hump overlies largely cartilaginous septum. In fact, it has been reported that 97% of dorsal humps lie caudal to the ethmoidal point. This anatomic relationship permits descent of both the bony and cartilaginous dorsum following resection of the cartilaginous septum. This anatomy is key to the mechanism of dorsal reduction associated with the subdorsal flaps discussed in this review.
Subdorsal Strip Resection
Goodale first described correction of a dorsal hump with what is now known as the push-down (PD) technique for bony vault management. He utilized endonasal root and lateral osteotomies, along with dorsal cartilaginous septal wedge resection, to lower the entire bony-cartilaginous complex as a single unit into the nasal cavity medial to the maxilla. , Lothrop described what is now known as let-down (LD) technique in which wedge resections of the nasal bones were added to allow the bony vault to rest on the maxilla. Both of these methods involve resecting the immediate subdorsal septal cartilage to permit dorsal reduction.
The excision of high septal cartilage has also been advocated by recent preservation experts including Saban and Gola. , , Using this method, appropriate hump elimination is thought to be technically simpler and easier to visualize, and allows the option to abandon preservation, open the middle vault, and convert to a structural approach. This is because all septal cuts are made in the most superior subdorsal aspect of the cartilaginous septum, leaving the remaining septum intact with adequate subdorsal cartilage for traditional L-strut septoplasty and grafting if needed.
Beyond Subdorsal Strip Resection
Expanding on immediate subdorsal resection, several other approaches to the septum in preservation rhinoplasty have been proposed. Cottle described a low septal resection with disarticulation of the cartilaginous septum from the ethmoid plate and resection of immediate subdorsal ethmoid bone. This method may be helpful in repositioning anterior septal deviations, as the entire cartilaginous septum is disarticulated and re-anchored to the maxillary crest. Finocchi developed a modification of the Cottle technique coined Simplified Preservation Quick Rhinoplasty , or SPQR. Hallmarks of this technique include a swinging-door septoplasty with a vertical incision in the septum beneath the highest dorsal point, excision of a low cartilaginous septal strip, PD or LD osteotomies, and repositioning of the septum in the midline. This technique is particularly useful for to address a straight axis deviation and high septal deviations using a dorsal preservation approach. , One drawback of these techniques is the lack of septal cartilage available for harvest. In addition, inherent to the Cottle and SPQR techniques is keystone disruption beneath an intact dorsum, which may cause apprehension, though it remains a powerful method for septal repositioning.
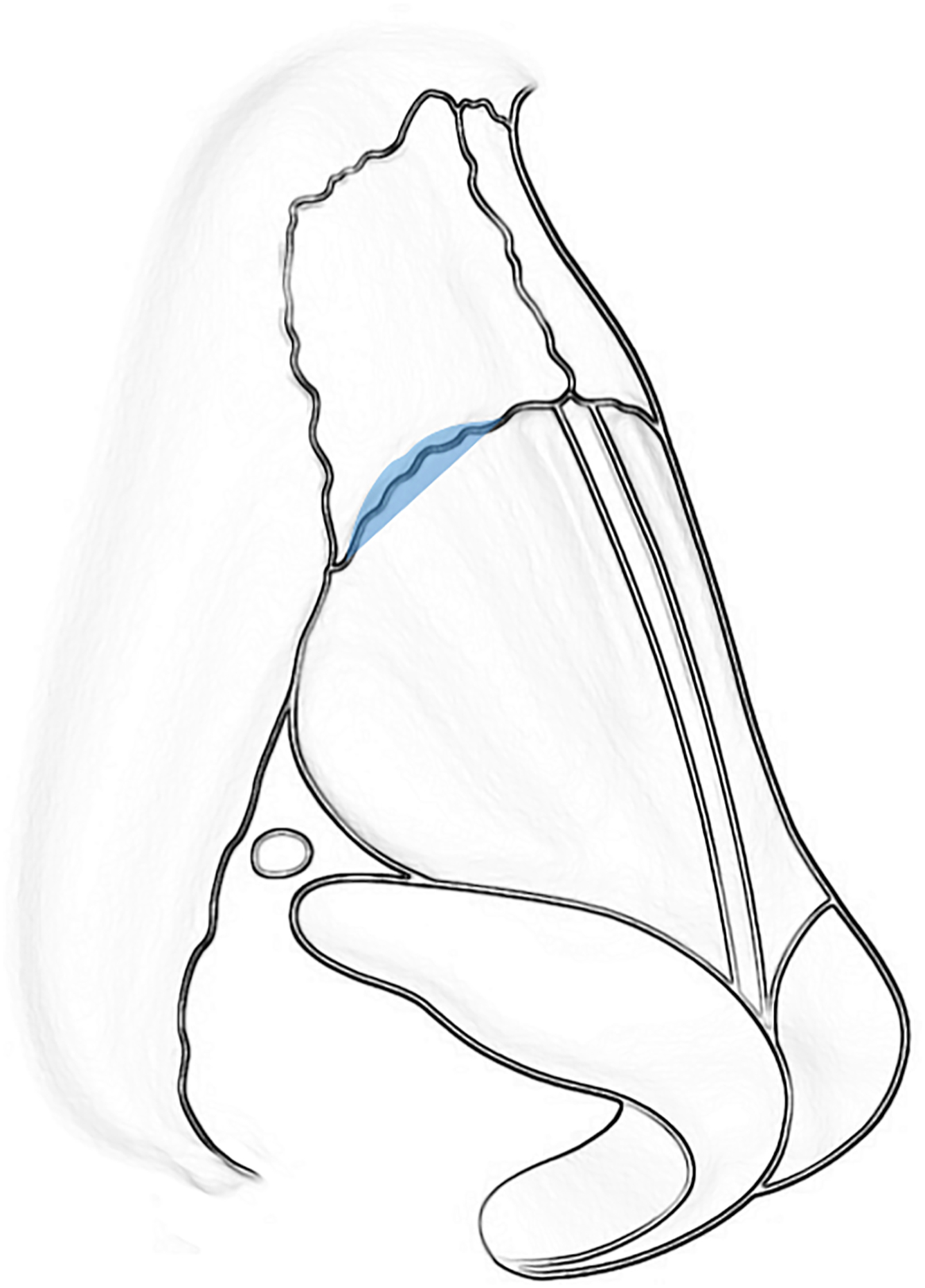
Several variations of intermediate septal cartilage resection between the immediate subdorsal and inferior septum have been described. These include: Ishida mid-septal resection, Neves Tetris Concept, most modified subdorsal strip method (MSSM), and Kovacevic Z-flap. Because a more generous portion of the subdorsal cartilage remains, these methods facilitate ease in anchoring the lowered dorsum to more inferior septal cartilage with suture. This stabilizes the dorsum in a lower position and allows for dorsal flexion, and may limit risk of middle vault deformity from scar contracture. All of these maneuvers include partial upper lateral cartilage release from beneath the nasal bones while preserving keystone attachments ( Fig. 2 ). This facilitates dorsal lowering and releases spring-like tension on the dorsum as it descends into the new, reduced position. This upper lateral cartilage release has also been termed the “ballerina maneuver”. Each of these septal approaches may accompany PD or LD DPR and are described here.
Ishida mid-septal resection
J. Ishida described a mid-septal, or intermediate , strip excision in which a rectangular segment of cartilage parallel to the dorsum is resected. This segment extends from the caudal septum to the bony-cartilaginous junction. It is best placed in an area of septal deviation in order to excise/correct the deviation, or 3 to 4 mm below the dorsum if the septum is straight. The remaining subdorsal strut may be sutured into its new flexed and reduced position, lateral osteotomies performed to allow descent of the nasal bones, and the bony hump removed down to the level of the new cartilaginous dorsum.
In his original publication describing mid-septal strip excision, Ishida reports satisfactory outcomes in 120 patients. One patient exhibited recurrence of axis deviation, 3 had a broad dorsum after 6 months, and 15% had hump recurrence. He notes that the width of the excised septal strip can be difficult to estimate and postulated that miscalculation of this led to cases of hump recurrence. The most optimal results were in patients with delicate structures including thin and fair skin, a small to medium size hump, and a narrow dorsum. Ishida describes the advantages of DPR with intermediate septal strip excision in a patient with this anatomy, advocating for its ability to create a natural-appearing middle third and avoid hump overcorrection, saddle nose deformity, and inverted-V deformity.
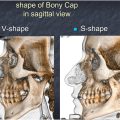
In a later publication from L. Ishida, a modification to this technique, in which the bony cap is preserved and lowered independently of the nasal bones, is described. In this modification, keystone osteotomies are performed to isolate the bony cap and maintain its continuity with the cartilaginous dorsum. The bony cap may then be lowered with the cartilaginous hump, and lateral/medial osteotomies performed to lower and narrow the nasal bones. This best preserves the dorsal aesthetic lines and prevents surface irregularities of the bony dorsum, and may be applied to a larger hump and wider dorsum due to isolation of the bony cap from the remainder of the independently-addressed nasal bones.
The Ishida mid-septal excision is commonly accepted as one of the first modifications to the classically described immediate subdorsal resection and low septal resection. This method preserves a subdorsal strut of cartilage and paved the way for several additional subdorsal approaches to the septum in DPR, which are reviewed as follows.
Neves tetris concept
Neves initially described an intermediate subdorsal septal resection approach in which a strip of intermediate subdorsal septal cartilage and bone is resected from the caudal septum superiorly to the transverse osteotomy site, parallel to the dorsum. A remnant 5 to 8 mm of subdorsal cartilage beneath the upper lateral cartilages remains to allow suture fixation. A vertical cut extending from this up to the rhinion is made to permit dorsal flexion and suturing of the preserved subdorsal cartilage to the inferior septum.
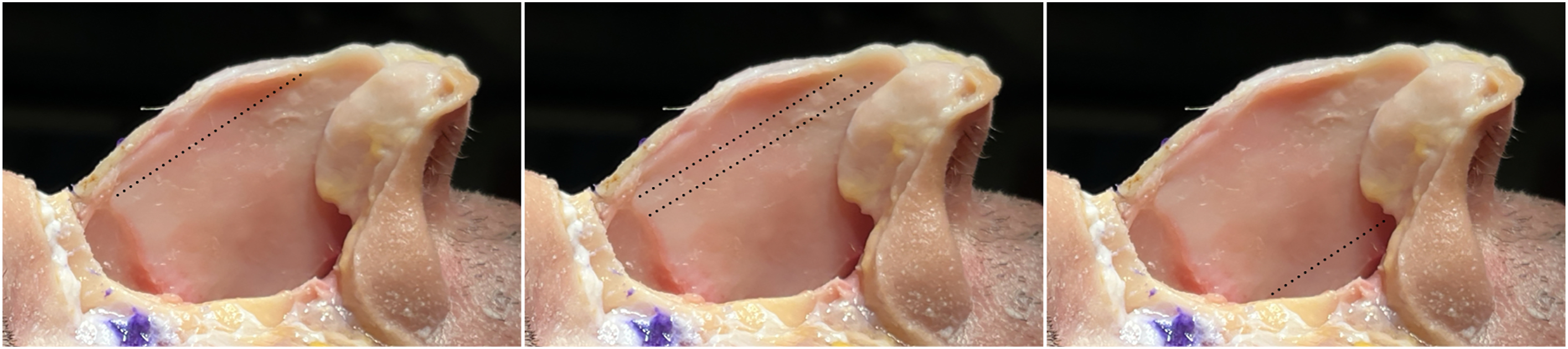
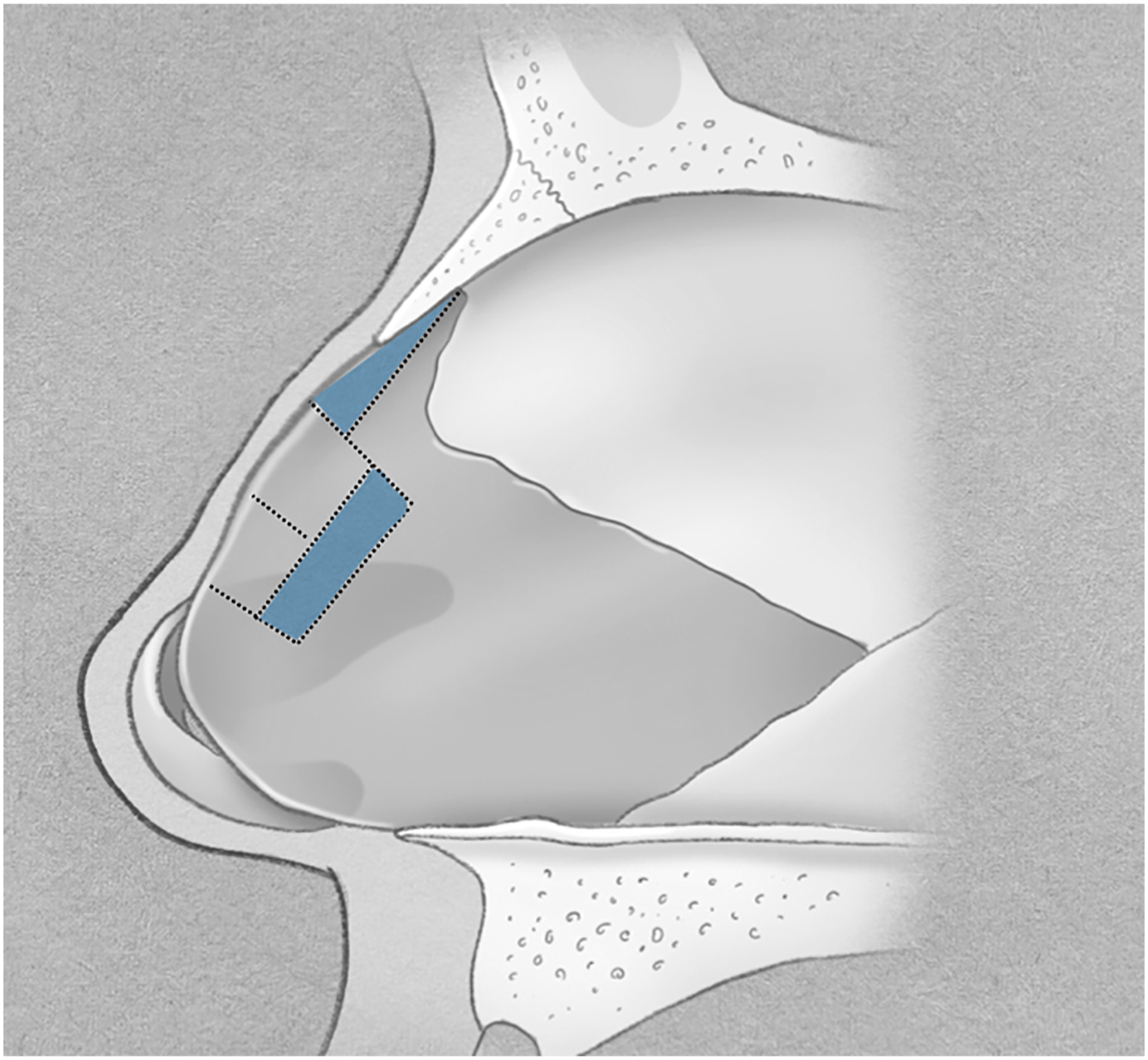
Evolving from this is Neves’ Tetris concept, in which a rectangular tetris block of cartilage below the rhinion is cut, flexed, and sutured to the anterior and inferior septum in 2 locations ( Fig. 3 ). First, relative to the dorsum, 2 perpendicular cuts and 1 parallel cut are made to create the tetris block. The block is 5 to 8 mm tall and extends from the caudal border of the upper lateral cartilages (ULCs) to the highest point of the hump. A triangular section of ethmoid bone is resected from the tetris block to the transverse osteotomy site to allow dorsal flexion. A trapezoid-shaped section of septal cartilage just beneath the tetris block, as well as a triangular section of cartilage along the caudal aspect of the block, is excised to allow the tetris block to flex and be secured to the remaining septum without overlap. If needed, the caudal septum may be trimmed to align with the new dorsal height.
Related posts:
 Alar Preservation Principles
Alar Preservation Principles
 Hybrid Dorsal Preservation Techniques
Hybrid Dorsal Preservation Techniques
 The Cottle Method and Modifications in Preservation Rhinoplasty
The High Strip Technique in Dorsal Preservation Rhinoplasty
The Cottle Method and Modifications in Preservation Rhinoplasty
The High Strip Technique in Dorsal Preservation Rhinoplasty
 Preservation Rhinoplasty—Outcomes in Dorsal Preservation Rhinoplasty
Preservation Rhinoplasty—Outcomes in Dorsal Preservation Rhinoplasty
 Expanding Indications to Dorsal Preservation Rhinoplasty
Expanding Indications to Dorsal Preservation Rhinoplasty
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


