High volume—the most common skin conditions seen in clinical practice;
High morbidity—skin disease that is contagious or can impact quality of life or the community; and
High mortality—life-threatening conditions that require prompt recognition.
thickness according to the body location. The hypodermis provides a layer of protection for the body, thermoregulation, storage for metabolic energy, and mobility of the skin.
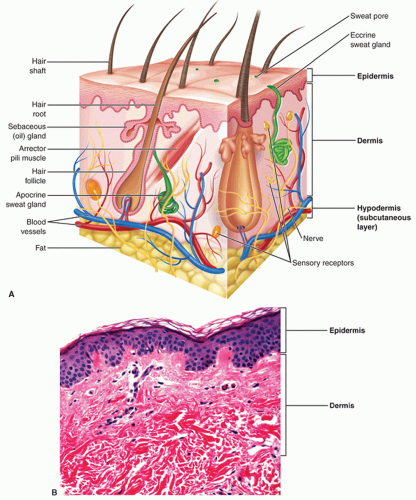 FIG. 1-1. Skin anatomy and histology. A: Anatomy of the skin. B: Corresponding photomicrograph of the skin showing the cellular distinction between the epidermis and dermis. |
hypohidrosis. Eccrine glands maintain an important electrolyte and moisture balance of the palms and soles.
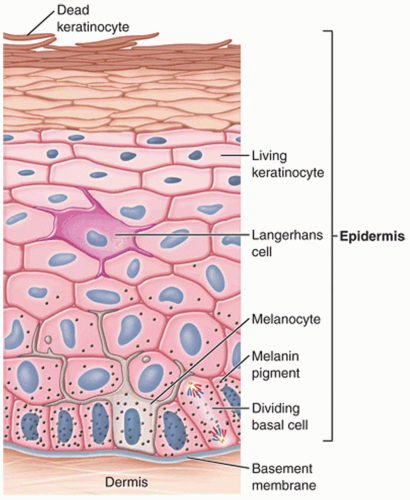 FIG. 1-2. Layers of the epidermis. |
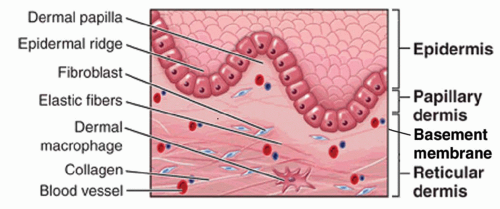 FIG. 1-3. Dermis. |
TABLE 1-1 Strata of the Epidermis | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


