46 Stick-and-Place Technique
Summary
Keywords: hair transplantation graft placing stick and place sharp implanter
Key Points
•The stick-and-place (S&P) technique involves making an incision in the skin, followed immediately with placing a graft into the incision with delicate forceps.
•The S&P technique can be used either for the entire procedure or only for part of the procedure to fine-tune an area (like the hairline) or to increase density.
•It usually requires two persons working in harmony to place each graft. It is more difficult to learn, but once mastered it is gentler and faster than using forceps in premade incisions.
•The main advantage is that bleeding and missed sites are less in the S&P technique.
•The main disadvantage is that it cannot be delegated, and it requires more staff.
46.1 Introduction
The stick-and-place (S&P) technique involves the surgeon making an incision in the skin with a sharp blade or needle, followed immediately afterward by an assistant placing a graft into the incision with delicate forceps.1,2,3 This is different than using premade incision (PMI) where all the incisions are made first and afterward the grafts are placed. The S&P technique has both advantages and disadvantages. The main advantage is that because sites are filled immediately, bleeding is less and it eliminates missed sites and piggybacking. This is useful when placing in between preexisting native hairs or grafts.
A disadvantage is that it in many places it cannot be delegated to technicians, which means more stress on the time and work for the physician. In addition, it usually requires two persons to place each graft, which increases staff requirement and may slow down the overall time of the procedure. The S&P technique can be used either for the entire procedure or only for part of the procedure to fine-tune an area (like the hairline) or increase density.
46.1.1 Stick-and-Place Technique Step by Step
Originally, when the S&P technique was first described by Limmer and later popularized by Seager,2 a single assistant performed the entire process. Today, the S&P technique is most commonly performed by two persons (a “sticker” and a “placer”) working together in harmony, each doing their part (see Video 46.1)2,:3
•Step 1: The “sticker” (usually the physician) makes the incision using a microblade. When the desired depth is reached, he or she either slightly twists or applies a little lateral pressure to the blade, creating a small “real” aperture in the recipient site. Sometimes, he or she will withdraw the blade slightly or about halfway before twisting (Fig. 46.1a).3
•Step 2: The “placer” gently slides the graft inside the incision, keeping it parallel to the blade. The blade can be used as a “shoehorn.” At this point, the placer usually has only inserted about a half of the graft into the site to avoid popping (Fig. 46.1b).
•Step 3: With the placer holding the partially inserted graft steady, the “sticker” then removes the blade (Fig. 46.1c).
•Step 4: Final adjustments are made to adjust graft flush with skin if needed.
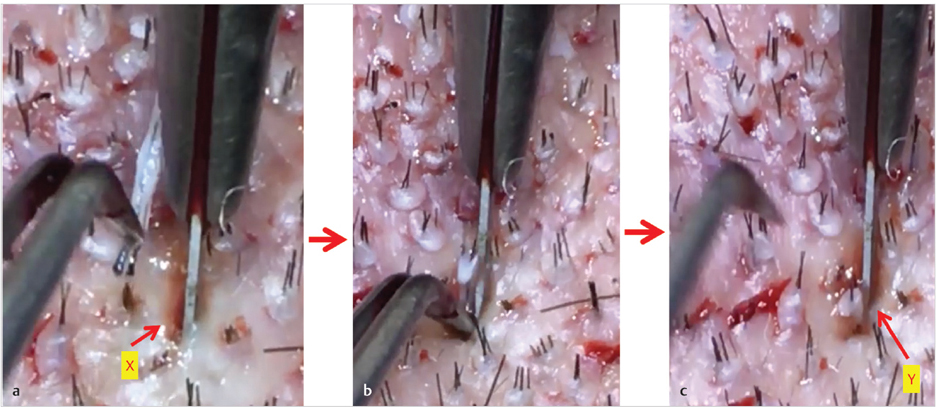
Fig. 46.1 (a) The “sticker” makes an incision with a microblade and (x) twist it slightly to create an opening. (b) The placer inserts the graft into the opening, sliding it down the blade like a shoe horn. The placer inserts only about one-third to one-half of the graft. (c) The sticker removes the blade, while the placer holds the graft with the blade point that has “hooked” the edge of the graft. If required, he or she will slide the graft further down into the incision with the tip of the blade.
Depending on the degree of popping and difficulty, this can be done in one of two ways:
•Option 1: In easy cases, with little popping, the placer simply uses the forceps to slide the graft down to its correct level, and then gently opens and remove the forceps.
•Option 2: In more difficult cases, the “placer” continues to hold the graft in place and wait for the “sticker” to use the blade tip to hook the graft at the point it exits the skin near the top. Once the graft is hooked (and stable), the placer removes the “forceps” and the “sticker” simultaneously uses the tip of the blade to slide the graft down to the desired level.
46.2 Pearls for Stick-and-Place Technique
46.2.1 Plan on Multiple Passes to Create the Pattern and Distribution
With the S&P technique, one should not create the final desired density and pattern of distribution in one pass for a few reasons. First, popping can be a problem when the S&P technique is done at high densities (40 follicular units [FUs]/cm2). Second, the exact final number of grafts that will be obtained is not known at the start of the procedure, thus making it tricky to plan the exact final pattern or distribution of grafts at the start. One has to be careful not to do too many grafts in one area and not have enough for other areas later. Multiple passes solve both these problems. On the first pass, you can create 70 to 80% of the final density and pattern. The final 30% can be used to fine-tune the pattern and increase density in critical areas. We also find that popping is less on the second pass after some time has passed for the grafts to settle down. It is important to use a brand new sharp blade to avoid popping.
46.2.2 Use Delicate Forceps with a Fine Tip
46.2.3 Match Incision Size to Graft Size
A benefit of the S&P technique is that physicians immediately see if the graft fits the incision. If not, proper adjustments can be made by either choosing a different blade size or instructing assistants to trim more precisely. For better precision, custom-cut chisel blades are used that differ in increments of only 0.05 mm. We typically use 0.65 to 0.7 mm for one-hair grafts, 0.7 to 0.8 mm for two-hair grafts, and 0.8 to 0.9 mm for three- to four-hair grafts. The 0.9-mm blades are usually only necessary for larger grafts found with white hair, splayed grafts, afro-textured hair, etc. We leave a slight 60-degree angle on our chisel blade because we find this tip is sharp enough to cut through the skin without popping, as well as “hook” the graft and slide it further into the incision. Some prefer to use needles for the S&P technique ranging from 19 to 22 gauge.
46.2.4 Depth Control
It is important to match the depth of the incision to the length of the graft. One of benefits of the S&P technique is that the physician gets immediate visual and tactile feedback about incision depth and can make corrections in real time while they are making the incision. However, it also helps measure and adjust blade length beforehand to gain more precise control over incision depth (Fig. 46.2).
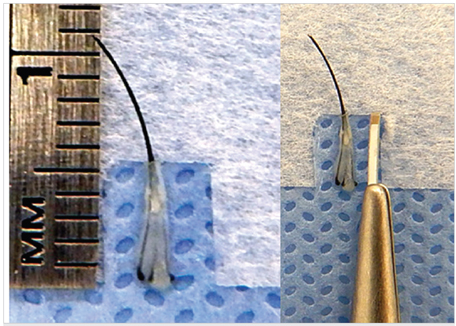
Fig. 46.2 Depth control. Adjust the blade depth in the handle, so the exposed blade length matches the length of the graft. With fine follicular unit excision (FUE) grafts, some limit the depth to about 0.1 to 0.2 mm less than the graft to prevent sinking.
Related posts:
 Methods and Techniques to Study Hair Cell Survival
Methods and Techniques to Study Hair Cell Survival
 The Patient with Minimal Hair Loss: Planning and Decision-Making
The Patient with Minimal Hair Loss: Planning and Decision-Making
 Hair Anatomy and Histology for the Hair Transplant Surgeon
Hair Anatomy and Histology for the Hair Transplant Surgeon
 Contact Management Software and Its Utilization as a Marketing Tool
Plugged in: How to Ensure That Your Practice Thrives (and Survives) in Today’s DigitalWorld
Contact Management Software and Its Utilization as a Marketing Tool
Plugged in: How to Ensure That Your Practice Thrives (and Survives) in Today’s DigitalWorld
 Recreating the Vertex
Recreating the Vertex
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


