Stevens–Johnson syndrome/toxic epidermal necrolysis
QUESTION 75
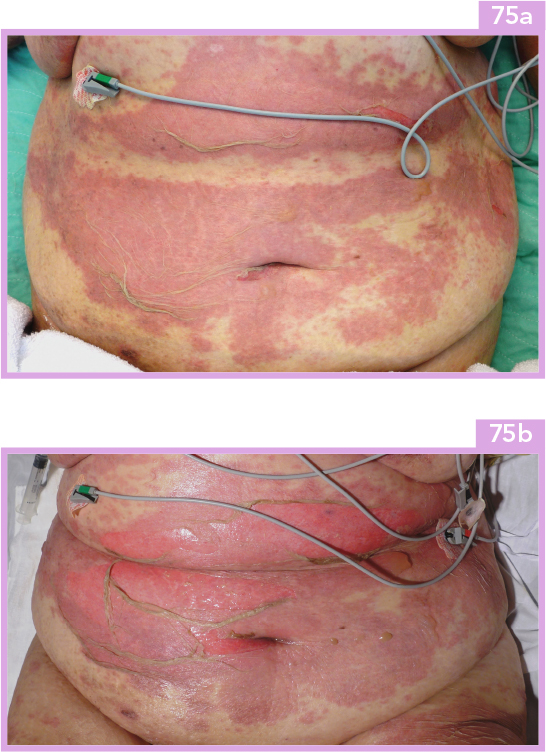
A 71-year-old woman presents to the emergency room with fever, malaise and a peeling rash. She has a history notable for poorly controlled diabetes mellitus and had started a course of sulfamethoxazole–trimethoprim and ciprofloxacin for cellulitis of the right foot 8 days ago. On examination, there are large confluent areas of dusky erythema, flaccid bullae and denudation. There are also oral mucosal erosions around and inside the mouth and bilateral conjunctival injection. She is admitted to the hospital and continues to develop large confluent areas of dusky erythema on the trunk and extremities with a cigarette paper-like texture (75a) with new blister formation and progression of denudation (75b, c) involving 70% of the total body surface area.

i. What is the diagnosis?
ii. What are the most common causes of this disorder, and what populations, if any, may be at risk?
iii. What are the complications and sequelae of this disease?
iv. What criteria can be used to predict mortality and what treatments are available?
Answer 75
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


