Children with cleft palate are at risk for speech problems, particularly those caused by velopharyngeal insufficiency. There may be an additional risk of speech problems caused by malocclusion. This article describes the speech evaluation for children with cleft palate and how the results of the evaluation are used to make treatment decisions. Instrumental procedures that provide objective data regarding the function of the velopharyngeal valve, and the 2 most common methods of velopharyngeal imaging, are also described. Because many readers are not familiar with phonetic symbols for speech phonemes, Standard English letters are used for clarity.
Key points
- •
Resonance disorders are common in children with a history of cleft palate. There may be hypernasality caused by velopharyngeal insufficiency (VPI). There may also be hyponasality or cul-de-sac resonance caused by obstruction in the vocal tract.
- •
Speech disorders are common in children with a history of cleft palate. There may be compensatory articulation productions caused by VPI or even caused by malocclusion if there was also a cleft of the primary palate.
- •
Differential diagnosis of the cause of hypernasality and/or nasal emission and also of abnormal speech sound production is critical in determining appropriate treatment (eg, surgery, speech therapy, or both).
- •
VPI is a structural abnormality and therefore requires surgical management.
- •
Velopharyngeal mislearning (including the use of compensatory productions caused by VPI or a history of VPI) is a functional disorder that requires speech therapy.
Anatomy and physiology of the velopharyngeal valve
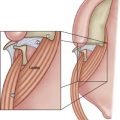
The velopharyngeal valve consists of the velum (soft palate), the lateral pharyngeal walls, and the posterior pharyngeal wall. These structures work in concert to open and close the velopharyngeal valve during speech.
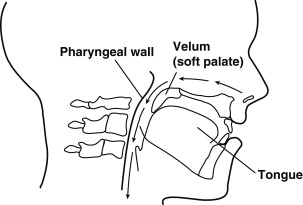
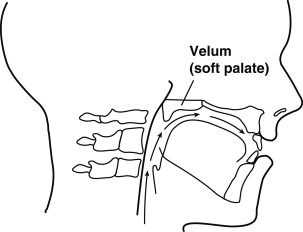
During nasal breathing, the velopharyngeal valve is open. The velum rests against the base of the tongue and the lateral pharyngeal walls are wide apart ( Fig. 1 ). This arrangement provides a patent upper airway for unobstructed nasal breathing. During oral speech, the velum moves in a superior and posterior direction to close firmly against the posterior pharyngeal wall (or adenoids in young children) ( Fig. 2 ). At the same time, the lateral pharyngeal walls move medially to close against the velum, or in some cases just behind the velum. Complete closure of the velopharyngeal valve is required for all vowels and most consonants. The exception is with the production of nasal sounds (m, n, ng), for which the velopharyngeal valve is completely open to allow nasal resonance. In connected speech, the velopharyngeal valve therefore opens and closes throughout an utterance based on the type of speech sound (oral or nasal) that is produced.
Anatomy and physiology of the velopharyngeal valve
The velopharyngeal valve consists of the velum (soft palate), the lateral pharyngeal walls, and the posterior pharyngeal wall. These structures work in concert to open and close the velopharyngeal valve during speech.
During nasal breathing, the velopharyngeal valve is open. The velum rests against the base of the tongue and the lateral pharyngeal walls are wide apart ( Fig. 1 ). This arrangement provides a patent upper airway for unobstructed nasal breathing. During oral speech, the velum moves in a superior and posterior direction to close firmly against the posterior pharyngeal wall (or adenoids in young children) ( Fig. 2 ). At the same time, the lateral pharyngeal walls move medially to close against the velum, or in some cases just behind the velum. Complete closure of the velopharyngeal valve is required for all vowels and most consonants. The exception is with the production of nasal sounds (m, n, ng), for which the velopharyngeal valve is completely open to allow nasal resonance. In connected speech, the velopharyngeal valve therefore opens and closes throughout an utterance based on the type of speech sound (oral or nasal) that is produced.
Velopharyngeal dysfunction
Normal velopharyngeal function depends on 3 basic components: normal structure (anatomy), normal movement (neurophysiology), and normal articulation learning.
When the velopharyngeal valve does not close consistently or completely during the production of oral sounds, this is often called velopharyngeal dysfunction (VPD). VPD is used as a general term that encompasses disorders of any of the 3 basic components of velopharyngeal function (structure, function, and learning). Other terms are used for more specificity as to the type and causation of VPD. For example, velopharyngeal insufficiency (VPI) is most often used to describe a structural defect that prevents complete velopharyngeal closure ( Fig. 3 ). Velopharyngeal insufficiency is the most common type of VPD because it can be caused by a history of cleft palate or submucous cleft. In contrast, velopharyngeal incompetence (also abbreviated as VPI) is used to refer to a neurophysiologic disorder in which poor movement of the velopharyngeal structures results in incomplete velopharyngeal closure ( Fig. 4 ). Finally, velopharyngeal mislearning refers to an articulation disorder in which speech sounds are inappropriately produced in the pharynx. As a result of this placement, the velopharyngeal valve is open, thus mimicking VPI during attempted production of certain speech.
Perceptual evaluation of velopharyngeal function
A speech pathology evaluation is indicated for all children with a history of cleft palate, particularly to rule out VPI. Although language development is assessed at a younger age, the speech evaluation for VPI is best done when the child has some connected speech and also at a time when the airway is adequate for secondary surgery, if needed. For most children, this is around the age of 3 years. A speech evaluation is also indicated both before and after secondary surgery for VPI.
The assessment of velopharyngeal function begins with a perceptual evaluation of the patient’s speech. During this evaluation, the examiner analyzes the acoustic product of velopharyngeal function in order to make inferences about the function of the velopharyngeal valve.
Speech Samples
When assessing speech, resonance, and velopharyngeal function, it is important to select an appropriate speech sample in order to obtain adequate information for a definitive diagnosis. The speech samples used to assess children with suspected VPD need to be developmentally appropriate in terms of both articulation and language. Standardized (norm-referenced) articulation tests are available for comprehensive assessment of speech sound errors. In addition, the examiner usually elicits a variety of other speech samples, based on the child’s language developmental level and what is suspected. These samples may include repetitive syllables (with pressure-sensitive consonants combined with both low and high vowels), rote speech (ie, counting), phonetically loaded sentences (eg, Take teddy to town), and spontaneous speech. When errors are noted, the examiner typically does more focused testing, including tests of stimulability.
What is Assessed
The perceptual evaluation includes an analysis of various components of speech, including resonance, oral air pressure and nasal emission, speech sound production, and phonation. These components are further described later.
Resonance
Resonance is typically evaluated by listening to connected speech. If there is abnormal resonance, the speech pathologist must determine the type (eg, hypernasal, hyponasal, cul-de-sac, or mixed). This distinction is of utmost importance because the type of resonance determines appropriate treatment.
Patients with cleft palate often have hypernasal speech. Hypernasality is characterized by excess sound in the nasal cavity during the production of oral sounds. The speech is perceived as low in intensity, muffled, and unclear. Hypernasality is most perceptible on vowels, which are normally produced by altering oral resonance. There may also be nasalization of voiced consonants, so that oral phonemes (speech sounds) are perceived to be more like their nasal cognates (eg, m/b, n/d, ng/g). As a general rule, if nasal phonemes are heard more frequently than normal, or if nasal phonemes are substituted for oral phonemes, the resonance is hypernasal and VPI should be strongly suspected.
Because resonance disorders are not mutually exclusive, the speech pathologist assesses for other types of resonance deviations, which are also common in patients with cleft palate. For example, there may be hypernasality on oral sounds caused by VPI but also hyponasality on nasal sounds caused by a blockage in the pharynx. Hypernasality caused by VPI can also occur in combination with cul-de-sac resonance, which is the result of blockage at the exit of one of the resonating cavities (pharyngeal, oral cavity, or nasal cavity).
Although hypernasality is most commonly caused by VPI, it can also be caused by other factors, including a thin velum or a large oronasal fistula. Hypernasality can even be phoneme-specific because of the substitution of nasal sounds for oral sounds (ie, ng/l or ng/r) or habitual use of a high posterior tongue position on certain vowels.
Hyponasality is also commonly noted in patients with cleft lip/palate. This condition may be caused by a maxillary retrusion, a narrow pharynx, or even enlarged adenoids. Postoperative hyponasality is also a risk of surgeries to correct VPI.
Nasal emission
Patients with a history of cleft palate often have nasal emission. Nasal emission can occur with hypernasality, if the velopharyngeal gap is large, or without hypernasality, if the gap is small.
The relative audibility of the nasal emission can give a clue as to the size of the velopharyngeal opening. Nasal emission that is barely audible (or inaudible but causes consonants to be weak in intensity or omitted) suggests a large velopharyngeal gap. A smaller velopharyngeal opening causes more audible nasal emission than a large one because there is more resistance to the flow, and therefore more friction. Air that flows through a small velopharyngeal opening is released with increased pressure, which causes bubbling of secretions on top of the valve. The result is a loud and distorting nasal rustle (also called nasal turbulence).
If present, the examiner notes the occurrence of a nasal snort, which is produced most often with /s/ blends, and/or a nasal sniff, which is a friction sound that is produced by forcible inspiration. A nasal grimace commonly accompanies nasal air emission. This observation is important because it reflects the patient’s extra effort in attempting to close the velopharyngeal port.
The consistency of the nasal air emission is also tested. Nasal emission that occurs during the production of all pressure-sensitive phonemes suggests a large velopharyngeal opening, particularly if it is associated with hypernasality. Nasal emission that occurs inconsistently, but on all pressure-sensitive phonemes, suggests a smaller opening because the patient can close the gap with short utterances or with effort. In contrast, nasal emission that occurs consistently on certain speech phonemes, but not on all pressure-sensitive sounds, indicates that the cause is faulty articulation placement rather than VPI. This finding is sometimes noted in patients with no history of cleft or VPI. It is also common in patients with a history of VPI who used pharyngeal fricatives as a compensatory production for certain phonemes. Despite surgical correction of the VPI, nasal emission (and sometimes hypernasality) persists because of the abnormal placement.
Speech sound production
In assessing articulation (speech sound production), the speech pathologist records all speech sound errors, including substitutions, omissions, and distortions. The potential cause of the errors is also identified (eg, abnormal structure, apraxia [a motor speech sound disorder], phonological disorder, delayed development, or normal developmental error). When there are structural anomalies, such as VPI or occlusal anomalies secondary to cleft lip and palate, the speech pathologist also determines whether there are any obligatory distortions or compensatory articulation errors.
- •
Obligatory distortions occur when the articulation placement (the function) is normal, but the abnormality of the structure causes distortion of speech. Obligatory distortions secondary to VPI include hypernasality, nasal emission, and nasalized consonants.
- •
Compensatory articulation errors occur when the placement of production is altered in response to the abnormal structure. When VPI causes inadequate oral airflow for consonants, the patient may compensate by producing the sounds in the pharynx, where there is airflow.
It is important to determine the cause of each error or distortion, and particularly to identify obligatory distortions versus compensatory errors. This is important because the treatment is different depending on causality. For example, obligatory distortions do not require speech therapy. Once the structure is corrected, the distortion disappears. In contrast, compensatory errors require speech therapy, preferably after correction of the structure.
Phonation
Dysphonia is common in individuals with VPI. In particular, vocal nodules often occur in patients with a small velopharyngeal gap or a nasal grimace. This condition is thought to be caused by strain in the entire vocal tract with attempts to achieve velopharyngeal closure. In addition, breathiness is sometimes used as a compensatory strategy to mask the hypernasality or to mitigate the nasal emission. In addition, patients with VPI secondary to a craniofacial syndrome are at higher risk for laryngeal anomalies. Therefore, the speech pathologist listens for characteristics of dysphonia, including hoarseness, breathiness, roughness, glottal fry, hard glottal attack, strain, inappropriate pitch level, restricted pitch range, diplophonia, or inappropriate loudness. When present, these findings are often rated on a severity scale from mild to severe using the Consensus Auditory-Perceptual Evaluation of Voice (CAPE-V).
Low-technology Tools for the Assessment
There are a few low-technology tools that can be used to assist with the evaluation. The most common are discussed here.
Mirror
The examiner can place a dental mirror under the child’s nares while the child produces pressure-sensitive oral sounds ( Fig. 5 ). If the mirror fogs, it indicates nasal air emission. A problem with this test is that the mirror needs to be placed under the nose after the individual starts speaking and removed before the individual stops speaking to avoid fogging as a result of nasal breathing. Another disadvantage is that there is no way to know whether the nasal emission was consistent or just occurred on one phoneme. In addition, the clinician must be aware that when certain compensatory productions (eg, nasal fricatives) are present, mirror fogging may also result.