The past 3 decades has seen a steady, almost exponential, increase in knowledge of vascular anomalies. A useful biologic classification system has evolved. A careful physical examination augmented with refined imaging will yield an accurate diagnosis and set the stage for treatment. A multidisciplinary team can offer treatment options with some degree of predictability. One option is surgery, which can be fraught with numerous complications. This article focuses on surgical principles and technical pearls in the treatment of these unique problems involving the upper limb. If incorporated into routine management, these suggestions will improve surgical outcomes.
The past 3 decades has seen a steady, almost exponential, increase in knowledge of vascular anomalies. A useful biologic classification system has evolved. A careful physical examination augmented with refined imaging will yield an accurate diagnosis and set the stage for treatment. A multidisciplinary team can offer treatment options with some degree of predictability. One option is surgery, which can be fraught with numerous complications. This article focuses on surgical principles and technical pearls in the treatment of these unique problems involving the upper limb. If incorporated into routine management, these suggestions will improve surgical outcomes.
General considerations
Surgical treatment of vascular anomalies is neither for the timid nor the arrogant. A well-balanced approach that incorporates calculated risk and cautious execution is necessary; one that can only be cultivated with experience. The surgeon who devotes a practice to the treatment of these lesions is obligated to document meticulously and analyze critically; habits that will serve one well for life-long learning.
At the outset, it should be stressed that unless one amputates a limb, these lesions can never be absolutely eradicated. Persistence of the vascular anomaly is the rule, despite significant extirpative operations. This fact is important to consider during preoperative planning and future interventions.
The diagnosis and treatment of vascular anomalies is rapidly changing. Parents and patients must be kept informed about the natural history of the particular malformation, options for treatment, and new types of surgical, pharmacologic, and minimally-invasive interventions. Many children with significant venous malformations (VMs) are treated conservatively during childhood and present as teenagers requesting surgery. These decisions can be difficult, because both functional and aesthetic considerations must be considered. The authors have noted that both lymphatic malformations (LMs) and VMs tend to become more symptomatic in adolescent girls than boys. Contrasted are fast-flow lesions that are slow-growing, indolent, and insidious. Surgeons must provide a clear explanation of all potential complications and expected short- and long-term outcomes before any surgical treatment.
The surgeon who has the courage to treat difficult fast-flow lesions should also be prepared to amputate a symptomatic nonfunctional or painful digit or limb after unsuccessful attempts at palliation. Patients with severe pain will often request amputation of the affected part. Others may wish to persist despite a functionless parasitic limb or digit. The most difficult decisions are in young children who do not verbalize their pain, and some teenagers who have minimal tolerance to pain and have not adapted well to their limb malformation. In difficult lesions, amputation should be considered and discussed preoperatively. The reconstructive surgeon need not view amputation as a failure.
Although a comprehensive review of surgical complications is beyond the scope of this article, these include compartment syndrome, bleeding, wound dehiscence, infection, devascularization of a limb or digit, secondary contracture, tendon adherence, and pain secondary to nerve injury. Adherence to basic surgical principles as outlined in this article will minimize these potential problems. Large vascular anomalies involving any portion of the upper limb are not impossible problems. Surgical treatment is often the best remedy and should not be viewed as the last-resort option.
Principles
Surgical principles gain acceptance with time and must be periodically reassessed and refined, particularly in this rapidly advancing field. Principles should not be confused with surgical techniques that change frequently, and are modulated to a great extent by technology. Many of the following principles have evolved from the early operative experience with vascular malformations (especially the fast-flow types), which was punctuated with complications. These principles are briefly outlined in Box 1 .
Plan carefully before the operation
Place incisions strategically
Operate in a blood-less field
Use fine surgical instruments
Identify and tag important structures
Dissect discreetly, rapidly, and confidently
Avoid intraneural dissection
Close meticulously
Immobilize the extremity postoperatively
Follow the patient regularly
Preoperative Planning
Preoperative planning is the cardinal principle of surgical treatment. Most poor outcomes can be avoided by adhering to this principle alone. Planning should include correlation of the size, extent, and involvement of structures with physical examination and imaging. Imaging modalities include plain radiographs, ultrasound, MRI, and angiography. Before surgery on complex fast-flow lesions, a step-by-step plan of resection, including the approach and extent, must be determined and followed. Serial studies of growing children are often invaluable in showing the true extent of involvement of the extremity. However, the absolute extension of a VM, lymphaticovenous malformation (LVM), or arteriovenous malformation (AVM) may not be completely delineated by these studies, and intraoperative decision-making may be required once the true extent becomes visible. Despite this, it is critical for surgeons to abide (as much as possible) by the initial plan; straying from the plan may lead to a violation of uninvolved areas, an inadvertent injury to neurovascular structures, a waste of precious tourniquet time, and an incomplete excision.
For complex lesions, the authors have found it helpful to print the angiogram and label the nidus, shunts, and all large branches within that portion of the lesion to be excised. These scans should be displayed in the operating room for easy reference during the procedure. Other preparatory steps for fast-flow lesions include central venous and peripheral arterial monitoring, availability of fast-flow warmers and blood products for transfusion, and intensive care unit monitoring postoperatively.
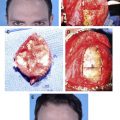
Placement of Incisions
Placement of incisions is important, particularly in children. When planning an incision, surgeons should consider exposure, blood supply, function, aesthetics, and future surgery. Incisions should be long enough to provide full exposure of the entire lesion ( Figs. 1 A and 2 ). Small incisions provide no surgical advantage, and risk injury to important structures. In the digits, a high mid-axial incision is preferred because it provides excellent exposure dorsally and volarly, can be used again, and is typically well hidden. Dorsal longitudinal hand and digital incisions are avoided if possible because they provide less exposure and are more conspicuous. Palmar incisions can lead to contracture if poorly planned; zig-zag incisions and those using normal skin creases are recommended.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


