Vascular anomalies are disorders of abnormal vasculogenesis or lymphogenesis. All types of vascular anomalies may involve the airway, causing varying degrees of upper airway obstruction as well as dysphagia and bleeding. Certain signs and symptoms may implicate airway involvement with a hemangioma or vascular malformation. It is necessary to distinguish a vascular anomaly from other airway lesions such as a congenital cyst. This is accomplished with imaging and endoscopy.
Vascular anomalies are disorders of abnormal vasculogenesis or lymphogenesis. Vascular malformations are labeled according to the vessel type including venous malformations, lymphatic malformations, capillary malformations, arteriovenous malformations, and mixed types (lymphatico-venous malformations). Vascular malformations may also be divided into low flow and high flow lesions. Low flow lesions include most vascular malformations, including capillary (port wine), venous malformations, lymphatic malformations, and combined lesions. High flow lesions include arteriovenous malformations (AVMs), arteriovenous fistula (AVFs), or aneurysms, which all have a high flow arterial pedicle. Venous malformations, lymphatic malformations, and AVMs are the most common vascular malformations to affect the aerodigestive tract, but are less common overall than hemangiomas. All types of vascular anomalies may involve the airway, causing varying degrees of upper airway obstruction as well as dysphagia and bleeding.
Certain signs and symptoms may implicate airway involvement with a hemangioma or vascular malformation. The most common pathology to affect the airway is a hemangioma and usually one with segmental distribution. The most common symptoms include biphasic stridor, recurrent croup, and retractions. Flexible laryngoscopy performed in the outpatient setting may show vascular staining of the endolarynx and may reveal a subglottic mass, but it may be difficult to appreciate small subglottic or tracheal hemangiomas on awake flexible laryngoscopy. It is necessary to distinguish a vascular anomaly from other airway lesions such as a congenital cyst. This is accomplished with imaging and endoscopy.
Airway imaging
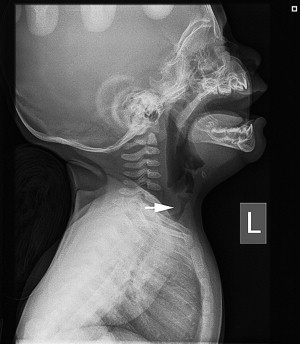
At the initial presentation of a child with stridor, plain films of the airway will show a tapered subglottic airway and a subglottic mass with a subglottic hemangioma and are very useful for assessing the subglottis ( Fig. 1 ). This is to be differentiated from subglottic stenosis or subglottic cysts. With these two pathologies, there is usually a history of intubation except with congenital subglottic stenosis, which is quite rare.
Sonography may be useful for defining vascular anomalies, but has limited resolution. Both contrast-enhanced CT/CT angiography (CTA) and MRI/MR angiography (MRA) are the most precise at defining vascular lesions and their extent of involvement in the aerodigestive tract. The injection of an arterial phase contrast agent is most important for demonstrating the vascular nature of the lesions and the extent of disease in the neck. However, one may have a limited view of the actual airway. MRI is most helpful for defining lymphatic malformations and determining microcystic versus macrocystic disease. Angiography is useful for determining the structure and blood supply of AVM, AVF, and aneurysm and allows for embolization before definitive surgery.
Operative endoscopy
Microlaryngoscopy and bronchoscopy (MLB) is an essential technique for confirming a diagnosis of an airway vascular anomaly such as a subglottic hemangioma. The technique is performed under general anesthesia with spontaneous ventilation. This allows for the most accurate assessment of the airway. First, flexible laryngoscopy is performed to study the dynamic characteristics of the larynx such as vocal cord mobility and epiglottic position, glossoptosis, and laryngomalacia. A flexible scope with side port suction is used to do this.
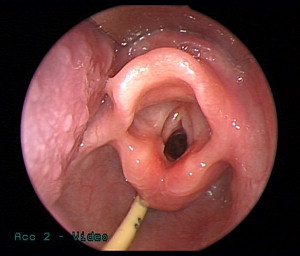
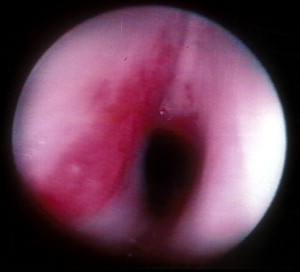
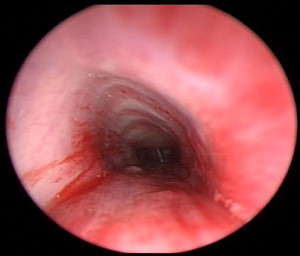
Microlaryngoscopy is performed with a rigid anterior commissure-type laryngoscope such as a Benjamin or Parsons placed in the vallecula ( Fig. 2 ) and used to expose the endolarynx and subglottic airway. This will reveal a subglottic hemangioma just below the vocal cords ( Fig. 3 ). Magnification from a Storz Hopkins telescope is used to visualize the subglottic airway and the scope can be passed down to the level of the carina. It is important to carefully look at the trachealis muscle in the back wall of the trachea for staining, fullness, and signs of vascular disease ( Fig. 4 ). Tracheal hemangioma may be subtle and its treatment is challenging.
Operative endoscopy
Microlaryngoscopy and bronchoscopy (MLB) is an essential technique for confirming a diagnosis of an airway vascular anomaly such as a subglottic hemangioma. The technique is performed under general anesthesia with spontaneous ventilation. This allows for the most accurate assessment of the airway. First, flexible laryngoscopy is performed to study the dynamic characteristics of the larynx such as vocal cord mobility and epiglottic position, glossoptosis, and laryngomalacia. A flexible scope with side port suction is used to do this.
Microlaryngoscopy is performed with a rigid anterior commissure-type laryngoscope such as a Benjamin or Parsons placed in the vallecula ( Fig. 2 ) and used to expose the endolarynx and subglottic airway. This will reveal a subglottic hemangioma just below the vocal cords ( Fig. 3 ). Magnification from a Storz Hopkins telescope is used to visualize the subglottic airway and the scope can be passed down to the level of the carina. It is important to carefully look at the trachealis muscle in the back wall of the trachea for staining, fullness, and signs of vascular disease ( Fig. 4 ). Tracheal hemangioma may be subtle and its treatment is challenging.
Management of hemangiomas affecting the airway
Hemangiomas are often seen in infants in the head and neck region and may involve the upper aerodigestive tract and airway. Involvement of the airway may result in varying degrees of upper airway obstruction as well as dysphagia and bleeding. Based on the distribution of the hemangioma, one may subclassify hemangiomas into focal, multifocal, or segmental based on the distribution characteristics. Focal implies a solitary lesion, whereas multifocal implies multiple. Segmental lesions occupy a dermatomal distribution. Most hemangiomas are solitary; however, the distribution may have an impact on the prognosis and the potential for airway involvement. Segmental hemangiomas are more likely to have involvement of the aerodigestive tract relative to solitary lesions, and multifocal lesions are more likely to simultaneously involve the liver or other areas of the gastrointestinal system.
When there is involvement of the airway, the symptoms are often stridor, croup, and respiratory distress. It is important to characterize the severity of the respiratory distress and the characteristics of the stridor. An infant with no history of intubation with a croupy (barky) cough and biphasic stridor localizes the lesion to the subglottic larynx. In the case of an infant with skin hemangiomas, the airway lesion would likely be a subglottic hemangioma. Following physical examination, it is necessary to proceed to imaging and endoscopy to confirm a diagnosis.
Hemangiomas may be classified by thickness as superficial, deep, or compound, as well as by distribution as localized, multifocal, or segmental. A localized hemangioma would involve a solitary lesion in the skin or airway, whereas multifocal includes 6 or more, and segmental involves a distribution in a known anatomic region such as V3 segment of the fifth nerve. Generally, airway symptoms are more common with segmental hemangiomas, and the so-called “beard distribution” in V3 is associated with a 20% to 30% involvement of the upper airway. The classic and most common finding is subglottic hemangioma, which is most often laterally based or less commonly posterior.
Less common sites affecting the airway include postcricoid, tracheal, mediastinal, thoracic, and esophageal. They may stain the posterior trachealis muscle (see Fig. 4 ). Airway symptoms include biphasic stridor and recurrent croup. Diagnosis may be suggested by history and lack of another cause of subglottic stenosis, such as prolonged intubation. Plain neck films may suggest the diagnosis.
Treatment of airway hemangioma depends greatly on the severity of symptoms, degree of airway obstruction, and the position of involvement in the airway. The treatment options for infantile hemangiomas of the airway are as follows:
- •
Observation
- •
Steroids
- •
Interferon: Historic – spastic diplegia
- •
Laser: CO 2 , KTP, Candela
- •
Tracheotomy: Discuss risk
- •
Open resection with or without cartilage augmentation
- •
Propranolol.
For mild cases with minimal or no symptoms, observation is all that is necessary. The size of a small hemangioma may not cause turbulent airflow or may involve nonendoluminal sites, such as the postcricoid region, which will cause no major airway symptoms. In such cases, no treatment is necessary, but close observation with flexible laryngoscopies in the ambulatory setting every 3 to 4 months is needed. However, it is important to understand that the symptoms may initially worsen as the hemangioma proliferates. Bilateral hemangiomas may impact the airway the most ( Fig. 5 ).
Mild cases or those that present with sudden acute airway symptoms may benefit from a short course of corticosteroids. This may be helpful during acute exacerbations, such as with upper respiratory infections. In addition, aerosolized racemic epinephrine may be used during acute exacerbations that can also occur with upper respiratory infections. Although racemic epinephrine can prevent an airway crisis, it may have rebound and is not a definitive treatment for airway hemangiomas. Corticosteroids decrease endothelial cell proliferation during the proliferative phase and hence they should be continued for most of this phase or there may be significant rebound. The typical treatment protocol would involve oral prednisone at a dosage of approximately 2 to 3 mg/kg/d for 4 to 6 months with a slow taper. Temporary side effects may include Cushingnoid appearance, behavior and mood changes, and rebound after discontinuation of steroids. Corticosteroids can also be administered intralesionally into lesions affecting the airway and may have more direct effects with less systemic side effects. Complications include bleeding and swelling after injection.
Recently, propranolol has been used to treat problematic airway hemangiomas. Before starting propranolol, one needs to get an MRI with gadolinium to rule out cerebrovascular disease and to avoid intracranial bleeds from rebound effects. Then an electrocardiogram is done to rule out arrhythmias and a fasting glucose is used to screen for hypoglycemia before starting and after the first 2 dosages. One should start at 0.5 mg/kg/d orally and work up to 2 mg/kg/d divided every 8 hours, but it can also be dosed every 12 hours. At the Children’s Hospital of Philadelphia (CHOP), we start propranolol as an inpatient, but with close monitoring, outpatient start is feasible as well. The drug is quite safe, as there appear to be few side effects. In our experience, the most common reported side effect is sleepiness or hypoglycemia. Exclusion criteria include arrhythmias, intracranial vascular malformations, and hypoglycemia. The mechanism of action of propranolol, a nonselective beta-blocker, appears to be capillary vasoconstriction, decreased expression of vascular endothelial growth factor (VEGF) and basic fibroblast growth factor (bFGF), as well as apoptosis of capillary endothelial cells. Denoyelle and colleagues in Paris, France, described 2 infants with subglottic hemangiomas who responded very rapidly to propranolol with no side effects. Both the subglottic regions responded right away to propranolol and avoided open surgery. Messner, at the 2009 Annual Meeting of the American Academy of Otolaryngology-Head and Neck Surgery, reported 6 responders of 7 patients tried on propranolol. The nonresponder was glucose transporter (GLUT)-1 negative. We have had 6 infants on treatment with 4 definite responders with no significant side effects. Our 2 nonresponders are GLUT-1 positive.
When pharmacologic means are not sufficient alone, lasers, such as CO 2 or potassium-titanyl-phosphate (KTP), can be used to treat surface hemangiomas in the airway. The CO 2 laser may work very well against small exophytic lesions in the subglottic airway. In the 1980s and 1990s, it remained a workhorse for subglottic hemangiomas; however, experience has shown that the recurrence rate with this technique is high. In addition, the laser may need to be used multiple times to achieve a stable airway because it treats only the surface and may not be effective at all for bilateral or circumferential disease. In addition, overaggressive use of the laser may result in subglottic stenosis. In the same way, the microdebrider, as demonstrated by Pransky and Canto, may be useful for focal lesions amenable to laser ablation. Although this technique has some of the same limitations as the laser, it is easier to set up than the laser and has less chance of injury from its use.
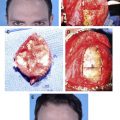
Open resection and cartilage graft augmentation has been reported as an effective treatment for subglottic hemangiomas unresponsive to more conservative treatments. The indication is a posterior or laterally based subglottic hemangioma that has failed steroids or propranolol. The procedure starts with a microlaryngoscopy, where the airway is assessed and secured with a small endotracheal tube orally. At this point, the patient may be given a course of intravenous steroids that may decrease bleeding during the resection.
The patient is positioned with the neck hyperextended and a transverse incision is made in the neck at about the level of the cricoid cartilage. A superior and inferior subplatymal flap is elevated to expose the laryngotracheal complex and the thyroid notch. This may expose extralaryngeal hemangioma in the neck ( Fig. 6 ). Stay sutures are placed on the cricoids, which is opened in the midline. The incision is performed with a Beaver blade and extended up to just under the anterior commissure. It is important to avoid violating the AC unless necessary. Posterior-based lesions are incised in the direct midline and the lesion is carefully dissected off the cartilage plate of the posterior cricoid ( Fig. 7 ) using otologic instruments such as the round knife, Rosen needle, and microtabe knife. An operating microscope may be prepped and used to facilitate visualization. Laterally based lesions may be approached by elevating a submucosal flap off the hemangioma from the laryngofissure down. When the lesion is resected completely, the flaps are sutured back into position using small vicryl. At this point, the airway is often stenotic and a small thyroid alar graft is harvested and used to augment the size of the subglottic airway ( Fig. 8 ). The graft is harvested from the thyroid alar and usually measures no more than 5 to 6 mm in length and 2 to 3 mm in width in a small infant, but this is enough to offset the stenosis. The wound is closed and the infant is kept nasally intubated for 5 to 7 days and then undergoes a microlaryngoscopy and bronchoscopy to evaluate the airway. If everything looks satisfactory, the patient is extubated the following day in the ICU. At CHOP, we have had 12 patients undergo this surgery, all with a remarkable resolution of their symptoms.