General Principles
In many ways, this is the “best of times” to practice medicine as a surgeon. We are at a time of unparalleled patient safety and at the cusp of remarkable advances in surgery including tissue engineering and tissue transplantation. We are also taking care of a patient population that is increasingly educated and inclined to take an active role in their health and health care. Conversely, it is also a time of great disappointment in medicine with frequent slipping standards of care and emphasis on the business aspects over the humanitarian aspects of medicine. The social contract between medicine and patients often appears broken with revenue-driven care models. This decline of professionalism roughly coincides with the advent of advertising in medicine. 1 The advent of widespread internet advertising that can replace surgical skills by the optimization of internet search functions has become a huge burden and disappointment for all specialties. Despite all of the turmoil, the Mohs repair surgeon continues to offer the opportunity to restore patients to full function after devastating and life-changing excision of skin cancers on their face; this can in many ways be considered the ultimate privilege in surgical practice.
The advantages of a surgical practice dedicated to post-Mohs reconstruction are many, including the majority of daytime cases with very little to no after-hours calls. The cases are on the smaller side and by no means fatiguing. The cases are almost all unique with different requirements and different expectations for “piecing the puzzle” together. Repaired properly, the patients are uniformly happy and pleased with their surgery and surgeon. The disadvantages are few and are manageable including the need for essentially year-round availability for patient care, as well as patient populations with significant comorbid diseases that require special attention and management.
In establishing a practice dedicated to post-Mohs surgical repair, one needs to fully understand the role that the surgeon will serve to the Mohs practitioner. Basically, the repair surgeon needs to fully and competently “take care of” the post-Mohs resection patients. This puts the onus on the repair surgeon to provide safe, effective repairs and render the patient uniformly happy with the repair, as well as the repair process. Full commitment to reconstruction patient care is required. The plastic surgeon that has no real interest in Mohs repair and is merely biding his time until he can either establish a cosmetic practice or is intending to convert Mohs patients to cosmetic patients or is using Mohs patients to “feed” a surgery center that is dedicated to cosmetic patients will have a short, bumpy career as an effective reconstructive surgeon. Additionally, post-Mohs patients are usually elderly and the repair surgeon who takes advantage of this lopsided patient–physician relationship with unreasonable surgical fees or co-pays or unreasonable schedule constraints or, worse, the surgeon who directs the patients to purchase overpriced wound or scar care products sold out of the surgeon’s office is no longer practicing medicine. He is rather engaged in extractionism and will have a short career as a Mohs repair surgeon.
Establishing a reconstructive practice to manage these patients entails the historical three As: Availability, Ability, and Affability. Availability or accessibility is paramount. The reconstructive surgeon must be readily available to the Mohs surgeon, as the requirements for a Mohs reconstruction are often not determined until the day of resection. The ability to rapidly provide scheduling for the surgical repair to avoid a patient waiting days or weeks is humane. The designated surgical facility should be in an easy geographic location and should be physically accessible to patients. The anesthesia team needs to understand the principles of anesthesia care for these patients, which is not always consistent with standard anesthesia practices, that is, these patients often will not require complex anesthesia workups for these small skin-only surgeries and in fact would be poorly served by standard “full preoperative anesthesia evaluation and workup” for minor surgical procedures. Also, current Medicare reimbursements for these types of cases are astonishingly low and a significantly large number of patients will need to be managed for a successful practice. Managing and effectively serving a large number of patients requires both the cooperation and the ability of the surgery center to accommodate last-minute scheduling, and schedule changes, as well as provide rapid turnover for these cases. As a rule, these patients are better served in an outpatient surgery center than in an inpatient hospital, as the majority are minor surgical procedures done in an hour or less and the patient should be able to return to their normal daily schedule afterward. Additional factors that go into making this work are standardized operating room sets, including prepackaged disposables, as well as standardized dedicated surgical instruments that can be rapidly “turned over” for reuse.
The operative planning for these patients first and foremost is predicated on the initial preoperative evaluation. It is not a requirement or even advantage that these patients are seen prior to their Mohs resection; however, accurate communication between the Mohs surgeon and repair surgeon is tantamount to ensure that complete excision has been performed prior to repair. The majority of decisions can be made regarding both the patient and the operative planning on the immediate visit prior to repair. That being said, it is incumbent upon the surgeon to understand that by the time the patient has had his or her Mohs resection and has found the surgeon for repair, he or she is at the end of a long day, is tired, usually has not eaten and is hungry, and often scared about the upcoming surgical process. The assessment of the patient’s expectations and comorbid disease and the assessment of the patient’s ability to comply with the planned repair process and postoperative requirements, especially if it is multistaged, all need to be determined with great accuracy. If a patient is woken early, not fed, placed in a dressing gown, he is in a vulnerable position and this can easily add 10 to 15 years of chronological age to his appearance, and reduce his functional status by many folds. The surgeon should very accurately assess the patient’s postoperative care requirements in order to provide a procedure that is appropriate. Understand that every patient does not need a multistaged surgical reconstruction (in many cases, this is a detriment), but this cannot become an excuse for the surgeon to develop a “good enough” or lazy approach to surgical repair. The caveat of restoring the patient’s appearance to normalcy and “one side matching the other side” should be the basis for every case in surgical planning and downgraded from there based only on the patient’s condition and requirements. The beginner’s practice of removing the Mohs dressing, looking at the defect, and then searching through surgical textbooks until a similar defect is found and utilizing that described procedure for the repair is both lazy and will provide suboptimal results. Rather, the development of basic principles based on anatomic location and character of the defect will provide the surgeon both comfort encompassing all varieties of the defect and improved aesthetic outcomes for the patient.
During this initial preoperative visit, surgical planning, as well as the patient’s ability to withstand the postoperative issues, which may require surgeries or multiple postoperative visits, needs to be appreciated. Many patients seen at large medical centers have traveled significant distances and just having to travel further may encompass significant hardships on the patient. These include costs and time commitments. Appropriate operative planning needs to also take into consideration a patient’s means of transportation to and from facilities.
The issue of current anticoagulation and cessation of preoperative anticoagulation has been thoroughly examined by Mohs surgeons and current practice is not to stop anticoagulation in the perioperative period. This needs to be ascertained by the surgeon as to whether this will adversely impact the repair. Although it is prudent to see the patient as soon as appropriately possible after the Mohs excision, the definitive surgical repair does not need to be performed that day. Oftentimes, a patient with a poor or a nonexistent preoperative workup that does require preoperative evaluation, or a patient with anticoagulation that needs to be off anticoagulation, or a patient with external or home constraints that need to be optimized prior to surgery, can be managed with the simple placement of a cellular tissue-based product (either dermal regeneration template or acellular dermis) and the wound can then be temporized and managed for up to a month with very little wound care or dressing care until the patient’s social or medical condition is optimized; however, it remains poor practice to leave a patient with an open wound pending scheduling per the surgeon’s convenience.
After surgery, attentive postoperative care is critical. Effective communication in the initial perioperative is essential. It is useful to have clear postoperative instructions printed on colored paper to be given to the patients as they are often discharged home with a stack of surgery center papers and it is helpful to be able to say refer to the “pink” sheet or a designated color sheet. As a note, the author has given all his patients his personal cell phone number for the last decade with very favorable results. The patients appreciate it and, with few exceptions, have been respectful of its use. An office call the first postoperative day to answer questions, provide follow-up, scheduling, etc., is mandatory. Great care is taken to normalize the patient’s activities postsurgery. There are very few reasons to limit patient’s aerobic activities postsurgery as increased heart rate or exercise will in no way affect postoperative healing; however, with grafts or flaps, we do limit the patient’s active strength training and picking up heavy objects until either the graft is assured taken and we are far enough away from the postoperative period that there is not risk for late hematoma. We make great effort to make dressings with no requirements for tape: either Surgicel for suture lines at risk of actively bleeding wounds or Xeroform for other wounds that become just a simple requirement of ointment. Also, stocking caps for the majority of scalp, forehead, and cheek defects are preferable to tape. We allow the patients to shower within the first 48 hours with no restrictions. If the patient is not seen preoperative, the first clinic visit is an ideal time to discuss the entire postoperative course including initial wound management, initial scar management, and final expectations for results. Postoperative photos of previous cases across all stages of wound healing are useful to set expectations.
The very nature of a Mohs repair practice is that fast efficient patient care needs to be practiced, but in a higher volume setting than in most plastic surgery practices. The physical location and the surgical facility need to be easily accessible by the patient and not overly cost prohibitive. An anesthesia staff that understands the special needs of these patients can safely execute a large number of cases and a dedicated nursing staff that can facilitate a rapid turnover are essential. The decision whether to undertake same-day repairs or next-day repairs is largely the surgeon’s and unfortunately the referring dermatologist’s preference. The advantages of next-day repairs are great. The patient is often already tired at the end of a long resection day and adding NPO (nil per os) status to their long day only makes it more difficult. Also, the ability of the Mohs surgeon to take postresection photographs and send them the night prior to the Mohs surgeon is exceedingly beneficial and prevents the removal of the Mohs postoperative dressing, which invariably results in bleeding in the immediate preoperative period. This allows the dressings to be removed in the operating room completely painlessly. The anesthetic choice for the vast majority of Mohs repairs is simple IV (intravenous) sedation with a brief period of propofol sedation, allowing the patient to wake up spontaneously after the painful local anesthetic injection. A fifty-fifty mix of 1% lidocaine with epinephrine and 0.25% Marcaine also with epinephrine is utilized in the majority of the cases with the advantage of Marcaine providing up to 4 hours of postoperative anesthesia. The surgical prep is a chlorhexidine prep, avoiding Betadine, and involves prepping the entire head with special attention paid to the ears and posterior scalp. The patient’s head is placed on a sterile drape and then the entire area undergoes a four-towel draping with great care to prep the same way each time, as well as prevent any tenting around the mouth or face. The use of prepackaged surgical supplies is exceedingly useful and ultimately is cost-effective and prevents waste. The choice of instruments again is the surgeon’s preference. A standard plastic surgery set can be utilized with the addition of individual instruments. For instrument sets that require frequent steam sterilization, the sharpness of fine instruments and scissors may suffer. Both are required for delicate tissue handling and should not be compromised. The solution is as follows: (1) sufficient quantity of sets to allow gas sterilization; (2) sufficient quantity of individual “peel packed” scissors to allow gas sterilization; or (3) frequent scheduled instrument service and scissor sharpening. However, the aggressive ability of the forceps and the sharpness of the scissors cannot be compromised on for successful results. The following five instruments have proven exceedingly useful over a decade of surgical experience. These include the following: (1) “cheap” microforceps that can be disposed of when they become dull. Normally used for microsurgical cases, these are very useful for rapidly removing embedded and retained sutures. (2) Neurosurgical watchmaker’s forceps can oftentimes be the go-to forceps for handling skin, particularly sewing in skin grafts. They have a long reach, are atraumatic, as well as having a needle holding a platform. (3) Neurosurgical Penfield no. 4 elevator has a cutting curette on one end and a flat elevator and can replace the majority of both caudal and the commonly used no. 9 elevators that are poorly shaped for Mohs repair. (4) The use of Lalonde forceps, which come in multiple sizes, are useful for grasping flaps. They are essentially small hooked forceps that act as tiny skin hooks and allow for the safe manipulation of flaps and skin edges with no long-term damage. (5) Finally, calipers are exceedingly useful both for setting excision diameters for skin lesions and for setting the uniform width of forehead flaps (▶ Fig. 1.1).
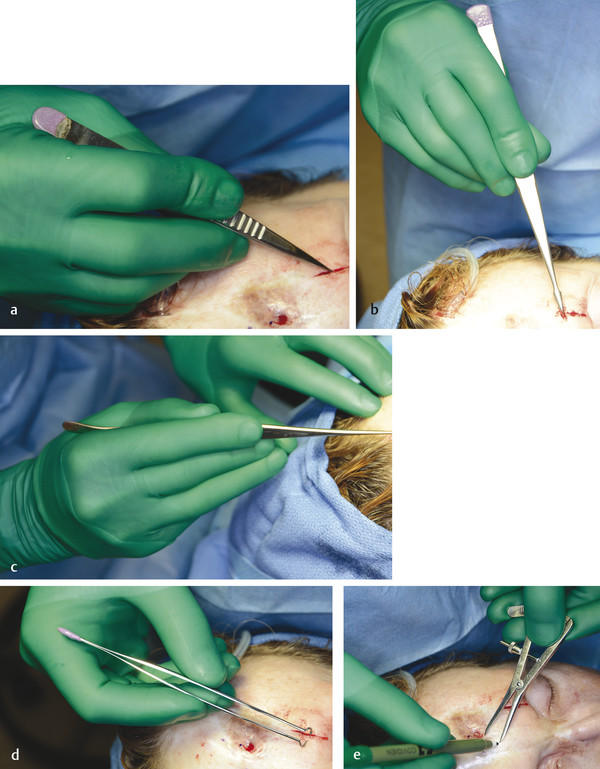
Fig. 1.1 (a–e) Microforceps, watchmaker’s forceps, Penfield elevators, Lalonde forceps, calipers.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


