58 Special Considerations for Anesthesia with Follicular Unit Excision
Summary
Keywords: anesthesia nerve block lidocaine toxicity conscious sedation ring block tumescent anesthesia
Key Points
•Effective use of local anesthetic agents and recognition and avoidance of anesthetic toxicity are critical in follicular unit excision.
•Patient relaxation is distinct from conscious sedation.
•Techniques to reduce discomfort during administration of local anesthetics are described.
•Regional nerve blocks and specific techniques for beard and body hair excision are discussed.
•Particularly since FUE procedures can be very time-consuming, it is imperative to frequently reassess and reanesthetize as necessary.
58.1 Introduction
In hair transplantation surgery, patient comfort and safety are of paramount importance. Whether a patient undergoes linear graft harvesting (“strip” surgery) or individual follicular unit excision (FUE) harvesting, the goals are the same: the patient should be relaxed and experience minimal to no discomfort. As the time required for graft harvesting is longer in FUE procedures, particular attention needs to be paid to ensure adequate duration of anesthesia throughout the entire donor harvesting process. Adequate initial anesthesia and periodic reinforcing of the anesthetized area to provide for a pain-free patient experience should be part of every hair transplant procedure.
Ensuring patient safety entails an awareness and understanding of each patient’s preexisting medical conditions. Medications taken by patients may interact with anesthetic agents and require alterations in surgical or anesthesia planning.
FUE hair transplantation is generally a lengthy procedure and is performed in an outpatient setting. Patient relaxation during the procedure is important and can be accomplished with oral agents; this is distinct from conscious sedation, which involves intravenous medication and requires continuous monitoring of oxygenation and airway status. There are physicians with the certification and training needed for conscious sedation and this is another option. Sedation with agents such as propofol requires monitoring by a board-certified anesthesiologist.
58.2 Anesthetic Agents
Local anesthetic agents fall into two types: amide or ester anesthetics. The most commonly used medications in hair transplantation surgery are the amide anesthetics, which have a rapid onset of action, greater potency, and longer duration of action than the ester agents. These include lidocaine, bupivacaine, articaine, mepivacaine, and prilocaine. These are metabolized in the liver and should be used with caution in patients with hepatic disease (Table 58.1).
Table 58.1 Commonly used local anesthetic agents in follicular unit excision
Agent | Dose (adult doses in patient without cardiac history; mg/kg) | Onset/duration |
Lidocaine with epinephrine (1 or 2%) | 7 | Fast/medium |
Lidocaine without epinephrine | 5 | Fast/short |
Mepivacaine without epinephrine (3%) | 5.5 | Fast/short |
Bupivacaine with epinephrine (0.5%) | 1.3 | Long/long |
Articaine with epinephrine (4.0%) | 7 | Fast/medium |
The ester anesthetics including procaine, tetracaine, and chloroprocaine are metabolized by plasma pseudocholinesterase and may be considered as alternatives for patients with true amide anesthetic allergy. Note that rapid toxicity can occur in patients with pseudocholinesterase deficiency.
Lidocaine HCl 1% is the most commonly used anesthetic agent in hair restoration surgery. The onset of effect is generally within 2 to 4 minutes, and duration of action can range from 30 to 60 minutes when used alone or 120 to 240 minutes when used in combination with low-dose epinephrine, which serves as a vasoconstrictor.
Symptoms of lidocaine toxicity can develop if the total daily dose (TDD) is exceeded. For lidocaine alone, the TDD is considered to be 5 mg/kg, while for lidocaine with epinephrine the TDD is 7 mg/kg. Note that some practitioners, including those performing tumescent liposuction, routinely exceed these recommended maximum limits (Table 58.2).
Table 58.2 Lidocaine total daily dose (TDD)
Body weight (kg/lb) | Lidocaine without epinephrine (5 mg/kg) | Lidocaine with epinephrine (7 mg/kg) |
50/110 | 250 mg | 350 mg |
60/132 | 300 mg | 420 mg |
70/154 | 350 mg | 490 mg |
80/176 | 400 mg | 560 mg |
90/198 | 450 mg | 630 mg |
100/220 | 500 mg | 700 mg |
110/242 | 550 mg | 770 mg |
Signs of lidocaine toxicity include central nervous system (CNS) effects such as a metallic taste, perioral numbness, restlessness, anxiety, altered mental status, and seizure. Cardiovascular effects of lidocaine toxicity may include hypotension, widened PR/QRS complex, atrioventricular (AV) dissociation, and cardiac arrest. While primary attention should be paid to avoiding toxicity, recognition of early signs of lidocaine toxicity is critical. Management of local anesthetic toxicity involves immediate attention to impending airway compromise, significant hypotension, dysrhythmias, and seizures.1 Treatment of local anesthetic toxicity may include the following: airway management, seizure suppression (benzodiazepines preferred), management of cardiac dysrhythmias, and for significant overdosage, lipid emulsion therapy may be required.
Bupivacaine is commonly used in hair transplant procedures. The 0.25% concentration may be used in field blocks, whereas the 0.50% concentration is more commonly used for peripheral nerve blocks. The onset of action is 5 to 10 minutes and duration when used alone or in combination with epinephrine may range from 120 to 240 minutes. The TDD alone is 175 mg; with epinephrine, the TDD is 200 mg.
Articaine, a newer amide anesthetic, is available as 4% solution with epinephrine either 1:100,000 or 1:200,000 and has been shown to be an effective and safe alternative to lidocaine with epinephrine,2 and this is the choice of some practitioners. Since clinical efficacy of 1:100,000 and 1:200,000 concentration of epinephrine was found to be the same, some authors recommend using the lowest concentration of epinephrine for increased safety.3
58.3 Ring Block
For many practitioners, the initial choice of anesthetic agent and technique is the same whether harvesting grafts via linear donor excision or individual FUE. A ring block utilizing lidocaine or articaine with epinephrine is performed. This may be followed or combined with bupivacaine to increase the duration of anesthetic.
Diminishing discomfort during local anesthesia is imperative and several techniques may be utilized. Buffering the lidocaine at a ratio of 1:9 with 8.4% sodium bicarbonate solution will increase the pH to a more physiologically neutral concentration. However, attempts to buffer bupivacaine solution will result in precipitation of crystals and should be avoided. Note also that buffered solution may be associated with greater postoperative swelling. This may have more clinical relevance in the frontal (recipient) area than in the donor areas. Alternatively, practitioners may choose to add epinephrine to the stock solution on the day of the procedure. This eliminates the need to change the pH as is necessary for stock solutions with epinephrine, and thus reduces the “stinging” without adding a buffer.
Vibratory distraction and pressure, that is, nearby physical stimulation, should be utilized to distract from the injection of the local anesthetic. The “gate control theory” of pain suggests that peripheral pain receptor impulses “should be slowed or abolished by any simultaneous input in the larger myelinated nerve fibers,”4,5 although this antagonism cannot always be shown. Using a fine gauge needle (30 g or smaller) can reduce initial discomfort. Application of topical anesthetic cream prior to injection may be appropriate is some settings.
Warming the anesthetic solution, as well as injecting slowly, will help reduce discomfort. Applying ice to the area to be injected may provide a modest amount of local anesthesia prior to injection. Initially injecting anesthesia at a slow, controlled rate and pressure with a microprocessor-controlled pump has been demonstrated to be less painful than hand injection.6
Note that injecting very superficially in the intradermal plane will result in more rapid onset and longer duration of anesthesia. However, this may be more uncomfortable than subcutaneous injection and can be performed subsequent to initial anesthesia. Injecting in a continuous wheal pattern, in which serial injections are started in the edge of the raised wheal from the prior injection, may be better tolerated than the “individual wheal” technique. Use of a blunt, flexible microcannula to reduce the pain of local anesthetics has recently been described (Fig. 58.1).7
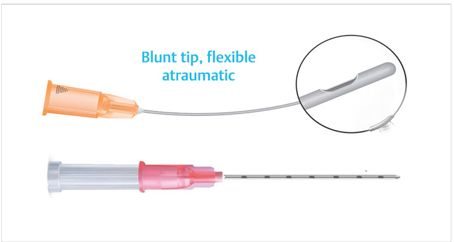
Fig. 58.1 Microcannula for injection of local anesthesia.
Related posts:
 The Patient with Minimal Hair Loss: Planning and Decision-Making
The Patient with Minimal Hair Loss: Planning and Decision-Making
 Hair Anatomy and Histology for the Hair Transplant Surgeon
Hair Anatomy and Histology for the Hair Transplant Surgeon
 Contact Management Software and Its Utilization as a Marketing Tool
Plugged in: How to Ensure That Your Practice Thrives (and Survives) in Today’s DigitalWorld
Contact Management Software and Its Utilization as a Marketing Tool
Plugged in: How to Ensure That Your Practice Thrives (and Survives) in Today’s DigitalWorld
 Recreating the Vertex
Recreating the Vertex
 Cosmetic Cover-ups and Hairpieces
Cosmetic Cover-ups and Hairpieces
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


