Dorsal Preservation Rhinoplasty encompasses various techniques that share the common goal of achieving a straight and smooth dorsum without the need for middle-third reconstruction using flaps or grafts. The Spare Roof Technique, classified as a surface technique, has shown consistent and reliable results backed by rigorous scientific evaluation, with its variations thoroughly tested over time. The authors provide a detailed overview of the current state-of-the-art in this technique as practiced globally, incorporating insights from over a decade of experience and refinement.
Key points
- •
The Spare Roof Technique (SRT) A and B are applied for nasal dorsum reduction, while the reverse SRT is utilized for augmentation rhinoplasty.
- •
The SRT A and B were developed through cadaveric, radiologic, and clinical studies assessing aesthetic and functional outcomes.
- •
Dorsal anomalies must be carefully diagnosed and fixed before any SRT A or B step.
- •
Surface Techniques, such as SRT A and B, in the era of osteo and chondroplasty can offer a universal approach to all primary rhinoplasties.
- •
Foundation techniques, such as Push/Let down, have limited indications and can lead to suboptimal outcomes if generally performed in all primary rhinoplasties.
| ASA | anterior septal angle |
| DALs | dorsal aesthetic lines |
| DP | Dorsal Preservation |
| FT | foundation technique |
| LDM | Lateral Division Maneuver |
| LKA | lateral keystone area |
| SAF | Septal Advancement Flap |
| SRT | Spare Roof Technique |
| SSNB | S-shaped nasal bone |
| ST | surface technique |
| ULC | Upper Lateral Cartilage |
| VSNB | V-shaped nasal bone |
Introduction
Dorsal Preservation (DP) has seen resurgence in popularity among surgeons in recent years, despite its origins dating back to its introduction by Goodale in 1899, further refined by Lothrop in 1914, and later popularized by Cottle in 1946.
The idea of preserving the middle vault and the good features of the dorsum is regarded as preferable to structural procedures. It would have been universally accepted if not for issues of surgical imprecision and loss of control. Fortunately, in the past decade, new concepts of nasal anatomy have emerged from cadaver studies and, more recently, accurate radiologic studies. , These concepts and findings have allowed new modifications of the early push-down/let-down techniques. Due to the evolution of techniques and a new understanding of anatomy, we are now in the era of advanced preservation rhinoplasty, and patients who were not considered ideal candidates for DP in the Cottle era may now be suitable.
Structural Versus Dorsal Preservation
The middle third is a transition segment between the bony pyramid and the tip, comprising only 1 T-shaped or M-shaped cartilage that, owing to academic and historical purposes, is divided into 2 Upper Lateral Cartilages (ULCs) and one Quadrangular Septal cartilage, with different thermo-mechanical characteristics. , Based on the integrity of the ULCs, there are 2 different ways to dehump a nose: the Structural Techniques (resection/reconstruction) and the DP Techniques.
The Structural Techniques consist of splitting the ULCs (among them) and the dorsal septum, separating this M-shaped segment into 3 parts. , It can be done by classical en bloc humpectomy or Component Dorsal Hump Reduction. In both cases, the dorsal hump is lowered by removing the leading edge of the nasal dorsum, which necessitates reconstructions with spreader grafts or spreader flaps, as well as osteotomies to close an open roof.
DP Techniques involve preservation of the leading edge of the nasal dorsum as the ULCs meet the dorsal septum with some potential modification of the bony cap. The middle vault is not opened as the dorsal hump is lowered by manipulating the nasal septum from below to align the profile. According to Toriumi, DP has experienced a revival because the method preserves the favorable anatomy of the upper two-thirds of the nose and minimizes the need for spreader grafts and spreader flaps.
Dorsal Preservation Techniques
Conceptually and structurally, 2 classes of DP techniques have been described for the bony dorsum: foundation techniques (FT) and surface techniques (ST).
FTs rely on dorsal impaction, which involves embedding the nasal pyramid into the face. This process necessitates impaction osteotomies that create a disruption between the skull and nasal pyramid (push down or let down).
STs focus on dorsal modulation where the hump is addressed superficially, allowing modulation of the middle vault without impaction osteotomies. Ishida Cartilaginous Push-Down (1999), Septorhinoplasty by Disarticulation described by Jankowski (2013), Spare Roof Technique A (2016), Spare Roof Technique B (2022), and Cartilage–only pushdown described by Kosins (2017) are some examples.
Recently, it was reported that STs are increasing in popularity and are considered more stable, predictable, and have a shorter learning curve.
Regarding managing the cartilaginous dorsum by DP, the dorsum (supported by the nasal septum) is modified by removing strips of cartilage at different levels, such as high-strip, medium-strip, and low-strip techniques. All techniques reduce dorsal support, allowing the dorsum’s height and shape to be modified.
Spare roof technique
The Spare Roof Technique (SRT) variations, A and B, are employed for nasal dorsum reduction, while the reverse SRT is specifically used for augmentation rhinoplasty. , , In 2016, Ferreira MG and colleagues introduced the SRT as a conservative middle-third preservation technique, enabling the surgeon to isolate the entire cartilaginous roof of the middle third without dividing the ULCs. This approach offers a refined method for treating the middle third, maintaining the structural integrity of the nasal anatomy, and minimizing the need for more invasive reconstruction.
Spare Roof Technique—Step by Step
The spare roof technique can be performed using a closed or open approach.
Regarding the bony cap, the SRT has been subdivided into 2 types: A and B.
SRT-A includes ostectomy of the bony cap. However, considering the clinical and surgical experience acquired over the years, for patients with V-shaped nasal Bones (VSNB) and up to medium S-shaped nasal Bones (SSNB), it would be possible to dehump the nose while preserving the Dorsal Keystone Area. Thus, based on a rational anatomic basis acquired experience with SRT-A, described by Ferreira MG and colleagues, and cartilaginous push-down with preservation of the bony cap, described by Ishida LC and colleagues, both authors designed a new technique named SRT-B or Ferreira-Ishida technique . This technique, named the Spare Roof Technique B (or the Ferreira-Ishida technique), is specially designed for patients with a dorsal hump and VSNB, preserves the bony cap, and ensures aesthetic brow-tip dorsal lines. In SRT-B, the treatment of the bony hump includes paramedian high parallel osteotomies just below the dorsal aesthetic lines (DALs) followed by inferior osteotomies to obtain a triangular shape of bone on each side of the bony cap.
Over time, SRT-B has been improved since it has been first described. Nowadays, SRT-B includes the following steps:
Step 1
Draw the desired dorsal brow-tip aesthetic lines on the skin’s surface, the pyriform aperture, the rhinion, the amount of triangular bone that must be taken out to allow pushing down the bony cap, and the transversal line at the beginning of the nasal hump. Evaluate the presence of any bony or cartilaginous dorsal irregularity that must be fixed with osteo and/or chondroplasty before any other step (in these cases, one must dissect the dorsum in that specific area).
Step 2
Hydro-dissect both lateral walls with a subperiosteal injection of 5 ccs of iced saline. Dissect both lateral walls through an intercartilaginous incision (with a Colorado® needle).
Optional
The dorsum preparation by osteoplasty or chondroplasty: dissect the dorsum only if there is any bony or cartilaginous defect. The most frequent bony anomaly that must be addressed is the kyphion edge of the S-Shape nasal bones, which can be managed with piezo or diamond burr. The most frequent cartilaginous irregularity is the noticeable shoulders that should be managed with a Colorado needle .
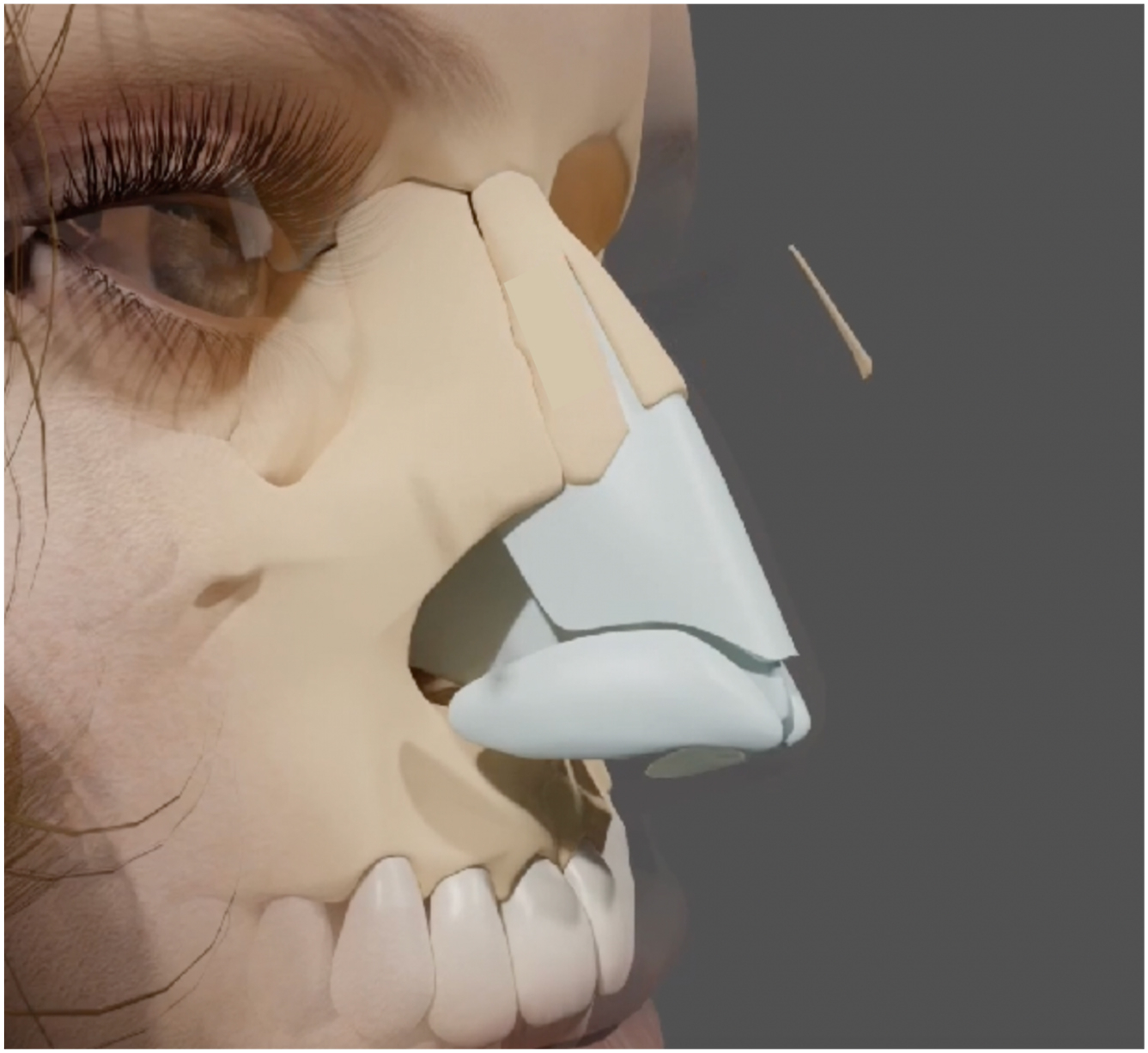
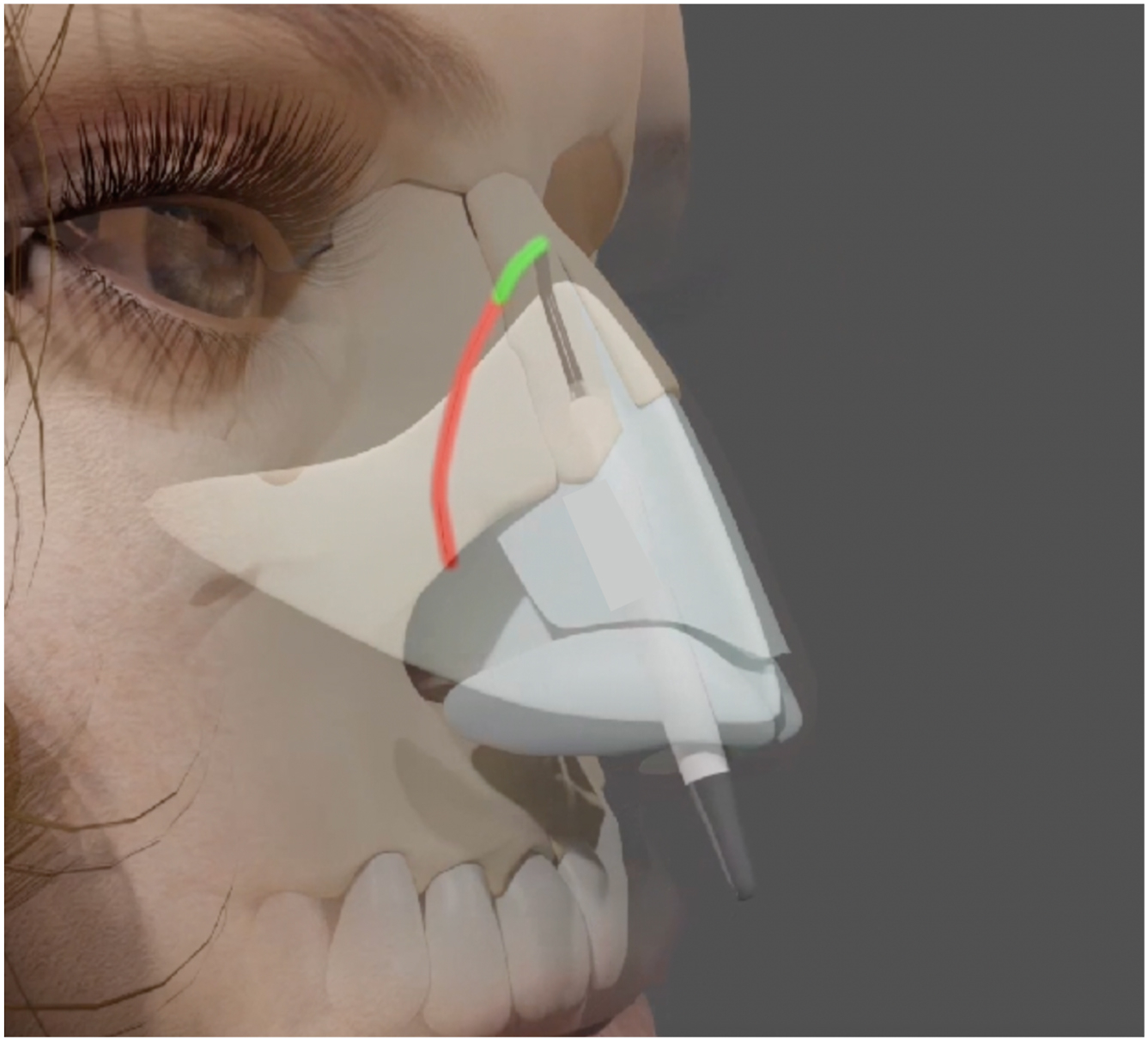
Perform the 2 triangular ostectomies (just out of the DALs): By endonasal (ultrasonic or osteotome), perform the paramedian high parallel osteotomies exactly below the marked brow-tip DALs. Then, perform the second group of lower osteotomies, until the E-point, to achieve a triangular shape of bone on each side of the bony cap. Perform the ostectomy of the mentioned triangular areas. Release the lateral keystone area (LKA) with a no. 15 blade as needed ( Figs. 1 and 2 ).

Perform Lateral conventional osteotomies—low-low-high—and leave the last 8 mm just with a simple piezo line to facilitate a real greenstick fracture at this ending level ( Fig. 3 ). These lateral osteotomies should be assisted with a proper bony forceps—the Ferreira Bony Forceps®. These 2 lateral osteotomies with the cephalic part in greenstick fracture are part of the Barnsdoors concept, where 3 contiguous greenstick fractures are combined ( Fig. 4 ).
Related posts:
 Understanding Dorsal Preservation Rhinoplasty
Understanding Dorsal Preservation Rhinoplasty
 Preservation Rhinoplasty—Outcomes in Dorsal Preservation Rhinoplasty
Preservation Rhinoplasty—Outcomes in Dorsal Preservation Rhinoplasty
 Subdorsal Flaps in Dorsal Preservation
Subdorsal Flaps in Dorsal Preservation
 Expanding Indications to Dorsal Preservation Rhinoplasty
Expanding Indications to Dorsal Preservation Rhinoplasty
 Combining Preservation and Structural Rhinoplasty
Combining Preservation and Structural Rhinoplasty
 Dorsal Augmentation with Preservation Concepts
Dorsal Augmentation with Preservation Concepts
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


