Soft Tissue Reconstruction With Propeller Flaps
Adam Jacoby
John T. Stranix
Pierre Saadeh
DEFINITION
Propeller flaps represent one of the most recent technical advances in perforator flap dissection.
Propeller flaps are especially useful alternatives to microvascular free tissue transfer when reconstructing distal lower extremity defects.
The perforator propeller flap can provide soft tissue coverage on all parts of the body despite its original and most common use for lower extremity defects. Its adipocutaneous composition and ability to be rotated up to 180 degrees provide an excellent source of thin pliable tissue along with a faster and relatively simpler dissection compared with free flap harvest.
To be considered a “propeller,” the flap must rotate between 90 and 180 degrees around its perforating vessels.
ANATOMY
Propeller flaps can be classified based on pedicle anatomy, either the type of pedicle supplying the flap or the pedicle position.
Island propeller flaps are skeletonized along the perforator vessels and allow up to 180 degree rotation with relative protection from pedicle kinking.
Nonskeletonized propeller flaps can be either skin- or muscle-based pedicled flaps where the dominant perforator is not skeletonized. Although operative times are shorter and there is less risk of perforator injury from dissection with nonskeletonized flaps, pedicle kinking is more likely— especially when rotated greater than 90 degrees (FIG 1).
Propeller flaps can also be classified as a central axis propeller (pedicle in the middle of the flap) or an eccentric axis propeller (at its periphery).
The arterial supply to the lower extremity is provided by the posterior tibial, anterior tibial, peroneal, descending genicular, and popliteal arteries with its venous supply largely mimicking the arterial network.
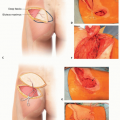
Perforators of the lower extremity form five vascular territories, separated by four organized rows of perforators originating within the intermuscular septa of the leg (FIG 2). Anterior tibial artery perforators are most often the smallest caliber.
PATIENT HISTORY AND PHYSICAL FINDINGS
Lower extremity defects are often caused by trauma, burns, or tumor extirpation. The defect size, depth, and location must be evaluated in addition to the surrounding skin quality. Additionally, exposed hardware (in the presence of orthopedic injuries), the bone, and the tendon must be taken into consideration when planning a durable reconstruction.
If the patient has severe peripheral vascular disease or insulin-dependent diabetes, atherosclerotic disease may prevent adequate inflow to the flap.
If the defect is from tumor ablation, the patient may undergo perioperative chemotherapy or therapeutic irradiation.
IMAGING
While computer tomographic (CTA) or conventional angiography is not required for surgical planning, CTA may demonstrate the presence and location of larger caliber perforators, which can aid in flap design.
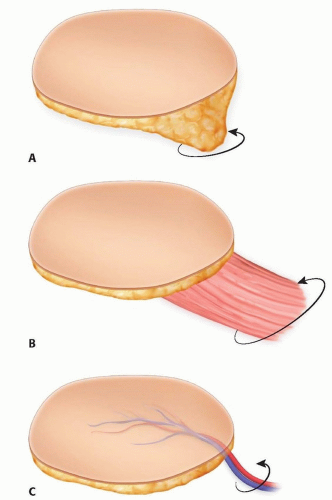 FIG 1 • Diagram of different pedicle dissections in propeller flap harvest; A. subcutaneous propeller flap, muscle-based propeller flap (B), and “true” skeletonized propeller flap (C). Note the relative bulkiness of the subcutaneous and muscular pedicles, placing them at higher risk for pedicle kinking with greater than 90 degrees of rotation. |
SURGICAL MANAGEMENT
Preoperative Planning
Unless contraindicated, general anesthesia with endotracheal intubation is preferred for these cases as the meticulous perforator dissection benefits from muscular paralysis intraoperatively. We routinely utilize preoperative Doppler detection of perforators for flap planning; however, it is not always necessary.
Although we find the use of a Doppler to be helpful, perforator detection may be confounded by superficial feeding blood vessels. In the setting of normal lower extremity arterial anatomy, intermuscular perforators are reliably found during intraoperative dissection, making preoperative Doppler identification a useful adjunct rather than a requirement.
If a Doppler is used, the length and width of the flap can be designed as follows:
The distance between the marked perforator and most distal aspect of the planned defect is measured; this distance is then transposed proximally, and 1 to 2 cm is added to determine the total length of the flap.
Half a centimeter is added to the anticipated defect width (to allow for contraction of the flap) to determine flap width (FIG 3).
Positioning
Location of the anticipated defect and dominant perforator dictate operative positioning as propeller flaps are useful in head-to-toe reconstruction.
For propeller flaps supplied by the posterior tibial artery system, supine positioning is used with the hip in abduction and leg externally rotated. Propeller flaps based off the peroneal system also require supine positioning, but a “bump” is placed under the ipsilateral hip. The hip and knee are then flexed and internally rotated.

FIG 2 • Schematic of lower extremity vascular territories and their feeding vessels. ATA: anterior tibial artery, PTA: posterior tibial artery, PA: peroneal artery. Small dots represent location of reliably found septocutaneous perforators within each angiosome.
For all flaps below the hip, a circumferential prep of the entire extremity is used routinely to ensure full visualization and allow intraoperative repositioning as needed. This also facilitates split-thickness skin graft harvest if required for donor site coverage.
For gluteal, sacral, or lumbar flaps, the patient is placed in prone position. The patient is sterilely prepped and draped widely—typically from the midthoracic region to the upper thighs.
Approach
When designing a propeller flap, it must be kept in mind that a skeletonized perforator can be rotated maximally 180 degrees around itself, whereas subcutaneous and muscle pedicled propeller flaps only allow for 90 degree rotation without kinking (see FIG 1).
As mentioned above, though preoperative Doppler use may help identify perforator locations, for skeletonized perforator flaps, the target perforator is only chosen after a suprafascial or subfascial dissection allows for visual inspection and confirms palpable pulsatility. An exploratory incision must be planned for adequate perforator exposure and examination which should not violate bail-out local flaps or an adjacent propeller flap supplied by a different perforator.
Predicted preoperative flap outlines (based off on-table Doppler examinations) often change after intraoperative dissection locates the dominant perforator.
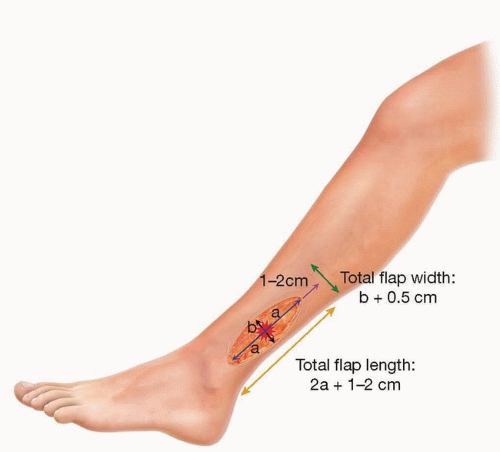
FIG 3 • The distance between the marked perforator (red star) and most distal aspect of the planned defect is measured (distance a). This distance is then transposed proximally, and 1 to 2 cm is added to determine the total length of the flap (length = 2a + 1-2 cm). Half a centimeter is added to the anticipated defect width (to allow for contraction of the flap) to determine flap width (b + 0.5 cm).
Maximum size has yet to be described, but there are case reports of a 22 × 8 cm peroneal artery perforator propeller flap1,2 and a 19 × 13 cm posterior tibial artery propeller flap1 based off one perforator. Perforators off the anterior tibial artery are generally the smallest caliber in the lower extremity and require smaller flap designs accordingly.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree