22. Soft Tissue Fillers
Ashkan Ghavami, Miles Graivier
RELEVANT ANATOMY AND GENERAL CONCEPTS1,2
NOTE: This chapter is meant to discuss all current filler applications. We will concentrate on FDA-approved fillers and their most common clinical indications. Use in some anatomic locations may not be approved by the FDA or specifically advocated by the filler manufacturers.
FOREHEAD
■ Indications for fillers are mostly for filling lines.
■ Lines and deep furrows, particularly in glabellar region, may not be fully correctable with muscle chemodenervation alone.
■ Deep transverse lines may require fillers as adjuncts to botulinum toxin.
■ Volume is as much an issue here as in other areas.
PERIORBITA
Upper
■ Deep upper sulcus, either congenital or from aggressive fat removal through blepharoplasty, may require soft tissue filling.
■ Lateral “tail” of brow can be lifted slightly with soft tissue fillers, in addition to chemodenervation of lateral orbicularis.
Lower
■ Tear trough deformity: Medial groove from region of medial canthus to orbital rim
• Multifactorial in severity, relates to: Position of orbital rim, thickness of skin, pigment of skin, amount of medial fat in lower lid, characteristic of orbicularis retaining ligament (ORL), variation in orbicularis muscle insertion (tarsal, septal, and orbital portions), and insertion of orbital septum
• Good indication for soft tissue filling with small-molecule hyaluronic acid (HA)
■ Lower lid–cheek junction
• Severity varies.
• Depth of presentation varies from the tear trough/nasojugal fold toward the lateral orbital thickening.
• It is not necessarily related to position of ORL, orbicularis, or arcus marginalis.
• Position is relatively stable throughout facial aging.3
• Small-particle fillers can be very beneficial in rejuvenation.
MIDFACE
Malar Shape and Projection
■ Fullness in malar region from lateral zygomaticomaxilllary junction to the nasomaxillary region below the tear trough is very important in overall facial rejuvenation.
■ Fat compartments in this region are deep and superficial.
• Various depths require multilevel filling.
■ Cheek fold, when present, should be corrected for balance.
■ This is an excellent indication for large-molecule HA fillers and/or hydroxyapatite.
Nasolabial Fold
■ Cause not fully known: Severity may be related to dermal insertions of deeper fascial attachments and position of mobile lateral soft tissue against more fixed medial upper lip region.4
■ Depth and location vary.
• Multilevel filling can be useful.
■ Some upper-segment depth is natural and desired.
■ Overcorrection should be avoided.
LOWER FACE
Lateral Perioral Lines
■ Formed mostly during animation
■ When present on repose, good indication for filling
■ Usually lateral to lowest point of nasolabial fold
■ May require multilevel filling
Upper Lip Lines
■ Superficial lines extend radial (perpendicular) to vermilion border.
■ Skin resurfacing (laser versus peeling) and botulinum toxin, along with volume restoration and filling of each specific line, gives most optimal correction when lines are severe.
■ Vermilion-cutaneous junction and upper lip augmentation are usually required.
Lips (Fig. 22-1)
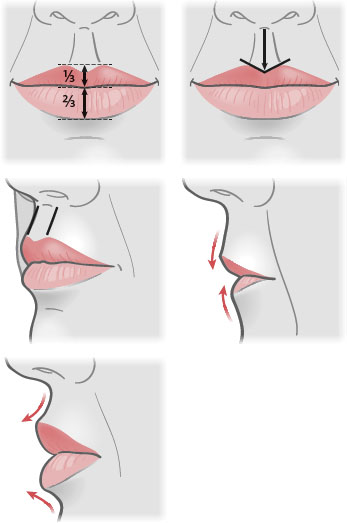
Fig. 22-1 Youthful lip characteristics.
■ Youthful characteristics
• Upper lip/lower lip height ratio should be ⅓:⅔.
• Cupid’s bow is sharp and well-defined.
• Full philtral columns
• Gentle concave sloping from nasal base and labiomental groove
• Oral commissures slightly upward in orientation
• Full medial tubercle
• Sharp white rolls (vermilion-cutaneous junction)
Labiomental Groove
■ Depth should be harmonious relative to nose-lip-chin projection.
■ Deep crease with cracked appearance would benefit from filling.
Chin Dimpling
■ Botulinum toxin along with filling can correct
■ Often only botulinum toxin required, however
Perimental Hollows (“Prejowl Sulcus”)
■ Good indication for deep-level filling with large-particle HA or hydroxyapatite
OTHER LOCATIONS
Nasal Contouring
■ Cephalad and/or caudal to a dorsal hump to blend and balance overall nasal appearance
■ Postrhinoplasty correction
• Nostril and alar imbalances
Scar Filling
■ Acne, posttraumatic, chicken pox
Crow’s-Feet
■ Chemodenervation is best treatment.
■ Once the skin is severely aged or thinned and separated from the underlying orbicularis muscle, then botulinum toxin is less helpful. Fillers are only rarely effective in this area when skin is thick and well adherent to the underlying orbicularis.
TIP: Consider the facial fat compartments5 and recognize/perform other complementary procedures that will blend facial zones and create overall facial youth and harmony through proper volume restoration.
INDICATIONS AND CONTRAINDICATIONS
FOLDS AND CREASES
■ As discussed previously, any crease, furrow, or line can be filled.
■ Caution should be used in filling lines in the forehead, because superficial placement is usually required, which can lead to vascular complications, ulcerations, and visible product.
■ Evaluate if botulinum toxin may be a substitute or if botulinum toxin–filler combination would be optimal.
■ Thickness of overlying skin/soft tissues is important.
• Lower lid–cheek junction and tear trough have thin skin that requires deep, conservative placement with a small-particle hydroxyapatite.
CAUTION: Calcium hydroxyapatite should NOT be injected in the lower lid–cheek junction and tear trough area.
• Nasolabial fold has thicker skin and multilevel injection technique with mutiple types of fillers may be used
VOLUME RESTORATION
■ Recent literature has helped our understanding of facial aging with respect to volume and position of soft tissue compartments.
■ Thorough knowledge of the fat compartments of the face and proper balance between fullness of these facial zones is essential.
■ Example: Malar fullness with submalar hollowing is a desirable aesthetic relation and a strong visual indication of youth.
■ Overcorrection can lead to an awkward “overdone” appearance.
ENHANCEMENT
Lips
■ An unnatural appearance should be avoided.
■ Adherance to the desired aesthetic proportions is vital.
NOTE: Some patients may demand overcorrection. Extreme caution should be used, as overcorrection should be avoided.
TIP: The lips are a vital and central portion of the face. It is a primary location that is subconsciously and consciously evaluated during social interactions. The lips evoke emotion, sensuality, youth, and vitality. Overcorrection in this region is commonly seen and makes many wary of soft tissue fillers. An incremental approach should always be used, with reevaluation from multiple views during injection.
CHIN PROJECTION
■ The appearance of minimal chin projection and fullness at the pogonion can be achieved with hydroxyapatite-based fillers.
PREINJECTION EVALUATION
HISTORY
■ Presence of a collagen-vascular disease process may interfere with healing at the injection site and compromise skin blood supply.
■ Any active skin or soft tissue inflammatory or infectious process should completely subside before injections.
■ Smoking may delay or interfere with healing and longevity of the product, especially if a collagen response is necessary for results.
■ Any immunocompromise indicates the need for extra caution.
■ Skin testing: Most fillers today do not require a skin test, however bovine collagen-based products can be used. (See the discussion on collagen-based fillers.)
AESTHETIC EVALUATION
Lips
■ Proper proportions should be understood, and all portions relating to improving lip aesthetics should be treated to optimize results.
■ Philtral columns, downturned oral commissures, and vermilion-cutaneous junction should not be ignored.
■ Volume and contour require treatment.
Lower Lid/Tear Trough
■ Evaluate depth and skin type.
■ Evaluate height of lower lid.
■ Evaluate requirement for multilevel filling.
■ Often, malar augmentation is also necessary.
Midface-Malar
■ Facial fat compartment locations should be assessed and understood.
■ Asymmetry should be documented. (One side is always wider than other.)
■ Middle cheek fold can be filled to blend the fat compartments.
■ This region is complementary with lower lid injections.
■ Multiple syringes are often required.
Lines/Furrows/Creases
■ The contribution of dynamic muscle motion, if any, is determined.
■ The best treatment is selected: chemodenervation, fillers, or a combination of both modalities.
■ Small static lines (periorbital and perioral) are a good indication for small-particle collagen.
INFORMED CONSENT
Should include, but not be limited, to the following:
■ Edema: Patients need to know timeline, because returning to their work and other activities is always important. Some fillers and locations produce more edema than others.
SENIOR AUTHOR TIP: Radiesse (Merz Aesthetics) injections deep in the malar region may allow return to work the same day whereas injections in the nasolabial fold may produce edema and erythema. Lips usually become edematous from the high vascularity.
■ Ecchymosis: Patients should not take aspirin, NSAIDs, and other blood-thinning medication for at least 1 week before injection.
■ Cosmetic outcome: As with any cosmetic procedure, the possibility of a poor cosmetic outcome or asymmetry should be discussed with patients.
• Lumpiness, in particular, should be discussed with patients.
• Contour irregularity
• Overcorrection or undercorrection
■ Allergic reaction/hypersensitivity: Rare hypersensitivity has been reported with all filler materials. However, bovine collagen–based products can produce a localized hypersensitivity and 1%-5% of negative skin test patients can produce an allergic reaction to facial injection.6 Previous hypersensitivity to a specific filler is a contraindication to repeat treatment.
• Cystic and granulomatous reactions are possible.
• Cystic abscesses have been reported.
■ Skin necrosis/ulcerations: Rare, but should be mentioned; more likely in poorly selected patients (e.g., cocaine abusers and those with autoimmune disease or collagen-vascular disorders); upper third of nasolabial fold near base of nose, and locations with watershed vascularity or thin overlying skin where superficial placement increases risk (e.g., glabella).
■ Pain/discomfort: Very temporary and easily minimized with proper technique; reduced by anesthetic block and icing. Prolonged discomfort or reaction at injection site may require corticosteroid treatment (injection or oral).
■ Recent laser or chemical peel treatment may increase the risk of inflammatory complications.
■ Infection: Rare. Risk is increased if active inflammatory or infectious skin process coexists at injection site(s). Delaying treatment may be needed.
• Herpetic reactivation
► Patients with a history of facial herpetic outbreaks should be pretreated for several days with oral antiviral therapy.
■ Tyndall effect or Rayleigh scattering: If injection is too superficial with any HA, a bluish discoloration will result (particulate bolus scattering shorter wavelength blue light).
EQUIPMENT
NECESSARY MATERIALS
Needles
■ Often provided in packaging
■ A 1¼-inch 27-gauge needle helpful for long, linear threading and for large areas such as the malar and nasolabial fold.
■ Otherwise, a ½-inch 27-gauge needle often used
■ 30-gauge needles good for superficial injections
Topical Anesthetic
■ Custom-compounded triple-anesthetic combinations can be special ordered from most pharmacies.
■ Requires application 15 minutes before procedure
■ Useful adjunct that should be placed before or at same time as local anesthetic blocking techniques
Local Anesthetic Block7
■ Agent: 1% lidocaine with or without epinephrine versus Septocaine
SENIOR AUTHOR TIP: Septocaine causes less discomfort.
■ Nerve block
• Posterior superior alveolar nerve (PSA)
• Infraorbital nerve (ION)
• Mental nerve
• Inferior alveolar nerve (IAN)
• Superior alveolar nerve branches
• Buccal branches (intraoral/mucosal)
Ice
■ Useful before and during injection
• Apply with pressure immediately before needle entry and between injections to prevent or minimize bruising and swelling.
■ May use ready-made iced rollers
■ Icing with pressure if bruise noted can minimize ecchymotic progression.
IDEAL SOFT TISSUE FILLER CHARACTERISTICS1
■ FDA approved
■ Biocompatible
■ Nonantigenic
■ Nontoxic
• Proven safety profile
■ Easy to use (i.e., filler material flows smoothly, needle and other equipment durable and does not fail easily)
• Long-lasting
NOTE: Permanence is not necessarily desirable. For example, some patients may not want their lips to be full for the rest of their life. As soft tissue and skin ages, delfates, and atrophies, permanent fillers will remain and look awkward.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


