Soft Tissue Coverage of Thigh—Free Flaps
Ulrich Kneser
Thomas Kremer
DEFINITION
Soft tissue defects of the thigh requiring free flap reconstruction are rare, because of a sufficient soft tissue envelope that frequently allows other reconstructive options such as splitthickness skin grafting, local random pattern, or pedicled flaps.
Exposure of functional structures such as neurovascular bundles, tendons, or bone may require reconstruction using free microvascular tissue transfer.
ANATOMY
Anatomy of the thigh is characterized by a sufficient number of strong muscles:
Anterior:
The quadriceps muscle (medial, lateral, and vastus intermedius muscle as well as rectus femoris muscle)
The sartorius muscle
Medial:
The adductor muscles (gracilis, adductor magnus, adductor longus, adductor brevis, and pectineus muscle)
Posterior:
Biceps femoris muscle
Semitendinosus muscle
Semimembranosus muscle
Perfusion of the thigh is maintained by the femoral artery and its branches:
Profunda femoris artery (with medial circumflex and lateralis artery)
Descending genicular artery
Popliteal artery
Peripheral branches of the inferior gluteal artery for the proximal dorsum
Major nerves of the thigh are:
The femoral nerve (quadriceps, sartorius, and pectineus muscle)
Obturator nerve (adductor muscles)
Sciatic nerve (posterior muscles of the thigh)
Venous drainage of the thigh is provided by deep veins and the saphenous vein.
PATIENT HISTORY AND PHYSICAL FINDINGS
Defects at the thigh may results from trauma, infection, or oncologic resection. Each of these entities should be evaluated and requires special focus during patient examination.
Patients with traumatic soft tissue defects of the thigh should be asked for the mechanism of injury. This may help to identify the true extent of the defect and concomitant trauma consequences.
Infections of the thigh should be evaluated for dynamics, systemic consequences (eg, fever, fatigue), pain, prior antibiotic treatment, as well as potential causes and infectious portals of entry.
The major goal in patients after oncologic resection is to evaluate prognosis, prior treatment, and adjuvant treatment options, since this information strongly influences therapeutic as well as reconstructive choices.
Additional important factors influencing reconstruction are patients’ demands: patients who were ambulating normally prior treatment may require more extensive reconstructive attempts than patients who are chair- or even bed-bound.
Inspection of the thigh in patients suffering from soft tissue loss should assess the extent and depth of the defect as well as exposed functional structures. Additionally, the surroundings of the defect should be carefully evaluated: scarring, tension, and former incisions should be noted. Prior radiation therapy may lead to wound healing disturbances and subsequent postoperative morbidity and should therefore be taken into account.
When free flap reconstruction is required, potential donor vessels should be evaluated. The distance from these vessels to the most distant part of the defect should be measured and significantly influences flap choices. In some patient, even more invasive strategies such as arteriovenous loops or bypasses may be necessary.
Patients should be asked for varicosity or prior venous surgery (such as venous stripping or bypass surgery).
IMAGING
Photographs of the defect should be performed including the complete thigh as well as detailed pictures focusing on the defect.
Conventional x-rays of the femur in two perpendicular views (anteroposterior and lateral) may show concomitant fractures or nonunions in traumatic cases, osteomyelitis after infection, or oncologic osseous lesions in oncologic patients.
Magnetic resonance imaging and computed tomography may reveal the real extent of the defect or sequelae of infection of the bone as well as soft tissue. However, both options should not postpone onset of treatment in special patients such as cases with necrotizing infections.
Radiologic examination of donor vessels is required in patients prior to microsurgery for thigh defects. MRI or CT angiographies are sufficient in most cases. The advantage of conventional angiographies in these patients is that endoluminal interventions are possible, if necessary.
Doppler or duplex ultrasound is indicated to evaluate the superficial venous system and for venous mapping if vein grafts may be required.
SURGICAL MANAGEMENT
Indications for free flap reconstruction at the thigh are relatively rare. Most cases can be managed using local random pattern or pedicled flaps as well as split-thickness skin grafting. However, extensive defects with exposure of functional structures such as bone, neurovascular bundles, or tendons may require free tissue transfer.
Another reason for microsurgical flap transplantation is radiation therapy. Tissues from distant donor sites that are not radiated may improve the healing capacity of irradiated wound beds. This is especially important because soft tissue sarcoma of the limbs most commonly occur at the thigh.1 Here, defect reconstruction using free flaps can even be indicated when primary wound closure would be possible with tension. In these patients, complications rates can be reduced when reconstruction with nonradiated flaps is applied.
Any reconstructive attempt should only be started when wounds are sufficiently debrided. No signs of infection or devitalized tissue should be present.
In some cases, vacuum-assisted closure (VAC) therapy can be performed to prepare wounds for soft tissue reconstruction.
Preoperative Planning
Different parameters influence the choice for various reconstructive options:
The aim of reconstruction (eg, palliative vs curative intention, limb salvage vs major amputation; ability to walk or just to sit)
Structures or functions requiring reconstruction, extent of the defect (eg, soft tissue loss, bone damage, muscle function, nerve injury)
Perfusion of the wound bed (eg, in patients with peripheral arterial disease, after radiation therapy)
The patients’ individual needs and compliance as well as concomitant diseases
Donor site morbidity
Adjuvant therapy options or further surgery
Another important information is the distance from potential donor vessels to the most distant part of the defect. If this distance is too long, the risk of partial flap loss (“where you need it most”) is increased. In these cases, arteriovenous loops or vessel interpositional grafts should be considered.
Patients with atherosclerosis should be evaluated by angiography and should be presented to vascular surgeons or interventional radiologists prior to surgery.
If multidisciplinary approaches are required (eg, osseous internal fixation, soft tissue reconstruction and/or vascular surgical interventions), a detailed preoperative discussion is required. The sequence and extent of different surgical steps, postoperative care, and operative strategy has to be considered. Here, interdisciplinary extremity boards similar to oncologic tumor boards have been shown to be very efficient.
Positioning
Patient positioning depends on donor vessels, flap choice, as well as additional surgical interventions (eg, osteosyntheses, vascular surgery, harvest of vein grafts).
Supine positioning allows:
Common flaps: anterolateral thigh flap, gracilis flaps, rectus abdominis myocutaneous flaps, tensor fascia lata flaps, vastus lateralis flaps, lateral arm flap, forearm flaps
Donor vessels: femoral artery and vein in the groin and adductors canal
Lateral decubitus position (FIG 1):
Common flaps: flaps from the subscapular system
Donor vessels: femoral artery and vein in adductor canal
In some patients, it is not possible to perform the complete procedure in one position (eg, when internal osseous fixation is required). Here, intraoperative repositioning may be necessary.
Approach
The surgical approach to defects at the thigh is defined by defect localization as well as extent and cannot be discussed here in detail.
Recipient vessels at the thigh predominantly are the femoral vessels. These can best be approached in the groin and the adductors canal.
In patients with unfavorable defect localization, microvascular anastomoses can be performed to arteriovenous loops (that can be performed in the same procedure or separately in prior procedures) or interpositional vein grafts.
If different approaches to the defect, vessels, and bone have to be combined, the surgeons should carefully discuss operative incisions in advance to prevent skin malperfusion.
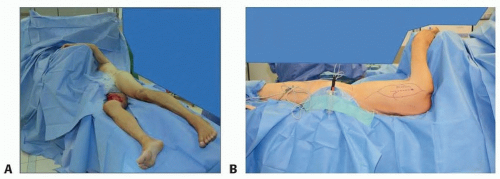 FIG 1 • The lateral decubitus position of patients allows exposure of the thigh and femoral vessels, if the contralateral leg is placed backward. A. Care has to be taken for the upper arm that has to be prevented from any compression to prevent compartment syndromes in lengthy procedures. B. Flaps from the subscapular system can easily be harvested.
Related posts: Fasciotomy of the Thigh, Lower Leg, and Foot Fasciotomy of the Thigh, Lower Leg, and Foot
 Bony Reconstruction of Foot and Ankle (Bone Grafts) Bony Reconstruction of Foot and Ankle (Bone Grafts)
 Vascular Reconstruction of Lower Extremity, Foot, and Ankle Vascular Reconstruction of Lower Extremity, Foot, and Ankle
 Tibial Reconstruction Tibial Reconstruction
 Femoral Bone Debridement Femoral Bone Debridement
 Amputation of the Lower Extremity: Above-Knee Amputation, Below-Knee Amputation, Through-Knee Amputation Amputation of the Lower Extremity: Above-Knee Amputation, Below-Knee Amputation, Through-Knee Amputation
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|