Soft Tissue Coverage of the Thigh—Pedicled Rectus Flap
Brock Lanier
Alex Wong
DEFINITION
Soft tissue defects of the thigh can involve critical anatomy including the neurovascular structures of the femoral triangle (i.e. common femoral artery, common femoral vein, and femoral nerve) and/or bone.
Prior infection, radiation, trauma, tumor resection, or other pathologies can render local or pedicled flaps from the thigh unusable for reconstruction. In such scenarios the pedicled rectus flap is a reliable workhorse for thigh defects.
The rectus flap is very versatile. It can be used as a pedicled muscle or myocutaneous flap. The available flap dimensions can range from a small segment of muscle to a large flap incorporating an extended skin component.1
ANATOMY
The rectus abdominis muscle spans the vertical length of the abdominal wall. It originates from the pubis, inserts at the fifth to seventh costal cartilage, and is situated in pairs along the paramedian axis of its anterior wall. It is a Mathes and Nahai type III muscle with two codominant vascular pedicles: the superior epigastric artery and the inferior epigastric artery (FIG 1).
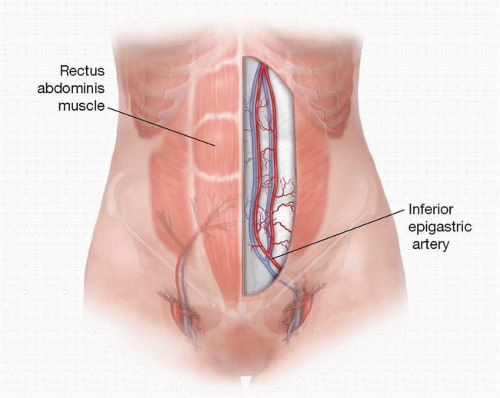
FIG 1 • VRAM clinical anatomy. The rectus abdominis muscle originates from the pubis and inserts at the fifth to seventh costal cartilage. It has codominant vascular pedicles: the superior epigastric artery and the inferior epigastric artery. The VRAM skin paddle must include periumbilical skin perforators.
In order to use the pedicled rectus flap for thigh reconstruction, the superior epigastric artery is transected and the flap is rotated maintaining the blood supply from the inferior epigastric artery.
Perforating branches from the inferior epigastric artery are concentrated around the umbilicus. As such, the periumbilical area should be incorporated into the design of any myocutaneous flap’s skin paddle.
If the periumbilical perforators to the skin are utilized, an almost infinite number of skin paddle designs are possible. Large (size) skin paddles can be transposed to the thigh defect if needed.2
PATIENT HISTORY AND PHYSICAL FINDINGS
Most soft tissue defects involving the thigh are associated with either trauma or cancer.
Focused examinations of the abdomen and lower extremity should be performed:
The abdominal examination should evaluate for previous surgical scars, the presence of abdominal wall hernias, and skin laxity if a myocutaneous flap is being considered:
Transverse midabdominal laparotomy scars indicate that the rectus abdominis was likely transected.
Low transverse scars associated with prior cesarean sections may or may not have violated the inferior epigastric pedicle.
Check the neurovascular status of the lower extremities. Trauma or surgery, particularly vascular surgery, involving the external iliac artery or common femoral artery, may have compromised the inferior epigastric pedicle.
IMAGING
Imaging is not mandatory but can be considered if the patient’s physical exam is concerning regarding the integrity of the inferior epigastric artery.
CT angiography can assess the pedicle and can concurrently evaluate the abdominal wall for occult hernias and other pathologies.
MR angiography and ultrasonography are other modalities that can also be considered.
NONOPERATIVE MANAGEMENT
Nonoperative treatment of soft tissue defects of the proximal thigh is limited, especially when critical structures of the femoral triangle or osseous structures of the lateral thigh are exposed.
Temporary coverage using vacuum-assisted wound care devices can be considered depending on the contents of the wound.
SURGICAL MANAGEMENT
Surgical management decisions include timing (immediate vs delayed reconstruction) and choice of the flap.
Flap options include local pedicled flaps of the thigh such as the anterolateral thigh flap, tensor fascia lata flap, gracilis flap, and sartorius flap.
Free flaps are also an option if appropriate regional options do not exist.
TECHNIQUES
▪ Flap Design
The size and depth of the soft tissue defect should be defined following tumor resection or wound debridement.
Critical landmarks include the symphysis pubis and the anterior superior iliac spine (ASIS), which defines the inguinal ligament.
The origin of the inferior epigastric artery is at the halfway point of the distance between the symphysis pubis and the ASIS.
The paramedian location of the rectus abdominis muscle is marked.
If desired, a template of the defect can be constructed (e.g., using wrapping paper from sterile gloves) to facilitate creation of the design of the skin paddle. It is suggested that the length of the muscle and the size of the skin paddle be slightly larger than the defect.
The donor site of muscle flaps will almost always close primarily.
The donor site of skin paddle of a myocutaneous flap should be assessed during flap design. A pinch test can ensure that the donor site will be able to close primarily.
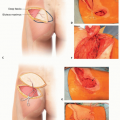
In pedicled flaps such as the rectus abdominis, the pivot of the flap about its vascular pedicle should be considered during flap design (TECH FIG 1).Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree