When looking at or communicating with an individual, the observer’s eyes flit between the individual’s eyes and mouth, which are the most expressive regions of the face. In fact, in considering features that were most influential to pleasing facial aesthetics, the appearance of the smile ranked second only to the eyes.2
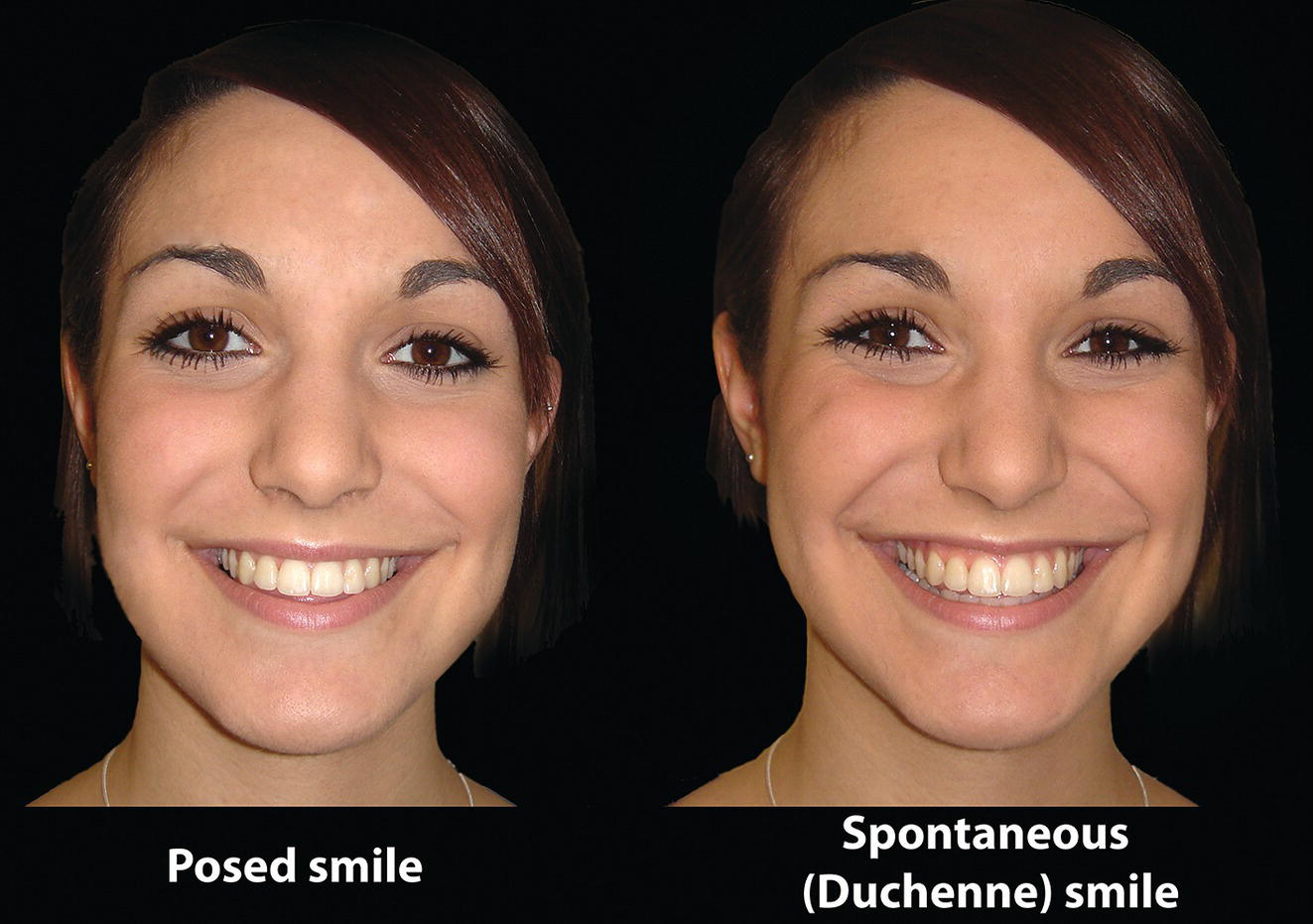
Two types of smile have been described in the scientific literature (Figure 23.1):
Posed smile: This is a voluntary smile, not linked with emotion, e.g. asking an individual to smile when taking a photograph. It is fairly reproducible. It may also be termed a non‐Duchenne smile, a ‘simulated’ smile or even a ‘false’ smile. The term social smile was used by the English poet Thomas Gray (1716–71).4
Spontaneous smile: This is an involuntary smile, often linked with joyous emotion. It involves larger facial movements, including squinting of the eyes (hence the term ‘smiling with the eyes’), flaring of the nostrils and maximum elevation of the lips. It may also be termed a Duchenne smile, or a ‘true’ smile.
The renowned English naturalist Charles Darwin (1809–1882), in The Expression of the Emotions in Man and Animals (1872),7 correctly emphasized that the clue to recognizing the true smile of enjoyment (the spontaneous or Duchenne smile) is the lowering of the lateral portion of the eyebrow. This is a subtle change, but together with lowering of the superior palpebral fold, it is a reliable sign that the outer fibres of orbicularis oculi have been contracted, and enjoyment is occurring. Ekman8 has demonstrated that crow’s feet wrinkles, and the bagging of the skin below the eye, can be produced by a strong action of the zygomaticus major muscle alone, without any contraction of the orbicularis oculi.
The generation of a smile
Two stages of smile formation have been described:9
Stage I: The levator muscles contract, thereby elevating the upper lip until resistance is met from the cheek fat present in the nasolabial folds.
Stage II: This involves further elevation of the upper lip against the resistance of the nasolabial folds and also elevation of the nasolabial folds themselves. Various muscle groups are involved in this movement (see Figure 3.5), including the levator labii superioris muscles, the zygomaticus major and the superior fibres of the buccinator muscle. The orbicularis oculi muscles may also participate in the effort to elevate the upper lip against the nasolabial fold, which produces the characteristic squinting of the eyes that accompanies a spontaneous smile.
Stage I is similar to the posed, non‐Duchenne smile; stage II is the spontaneous, Duchenne smile.
Clinical evaluation
Lip aesthetics
Aesthetic evaluation of the lips is an important part of the diagnostic process and is the starting point for the clinical evaluation of the smile. The acronym ‘LAMPP’ may be used to assess the lines, activity (function), morphology (height and form), posture and prominence of the lips. The aesthetic evaluation of the lips is described in detail in Chapter 17.
Lip lines
The lip lines represent the vertical position of the upper and lower lips in relation to the anterior dentition. The ‘ideal’ dentolabial relationship results when the upper lip covers approximately the upper two‐thirds of the maxillary incisor crowns at rest, with 2–5 mm maxillary incisor exposure; women tend to have significantly greater maxillary incisor exposure than men (Table 23.1).10 The interlabial separation is no more than 2–3 mm.
Table 23.1Incisor exposure at rest relative to sex
The upper and lower lips are brought into contact with little or no circumoral contraction, with the lower lip covering the incisal third of the maxillary central incisors.
The upper and lower lip lines must be evaluated with the patient in repose (resting lip lines) and in the dynamic state of speech and smiling.
The resting upper lip line may be defined as the vertical relationship between the inferior border of the upper lip and the incisal edge of the maxillary incisor teeth. The ‘ideal’ resting upper lip line is with the upper lip covering the upper two‐thirds of the maxillary incisor crowns at rest, with 2–5 mm maxillary incisor exposure.
A high resting upper lip line (sometimes termed a ‘high lip line’) leads to exposure of the entire clinical crown and associated gingivae of the maxillary incisor teeth, leading to excessive incisor exposure and sometimes an associated ‘gummy’ appearance at rest (see Figure 17.6).
A low resting upper lip line (sometimes termed a ‘low lip line’) leads to exposure of less than 2 mm of the maxillary incisor crowns. The maxillary incisor display may be non‐existent at rest and in extreme cases, in speech and in smiling (the ‘no tooth’ smile) (see Figure 17.7).
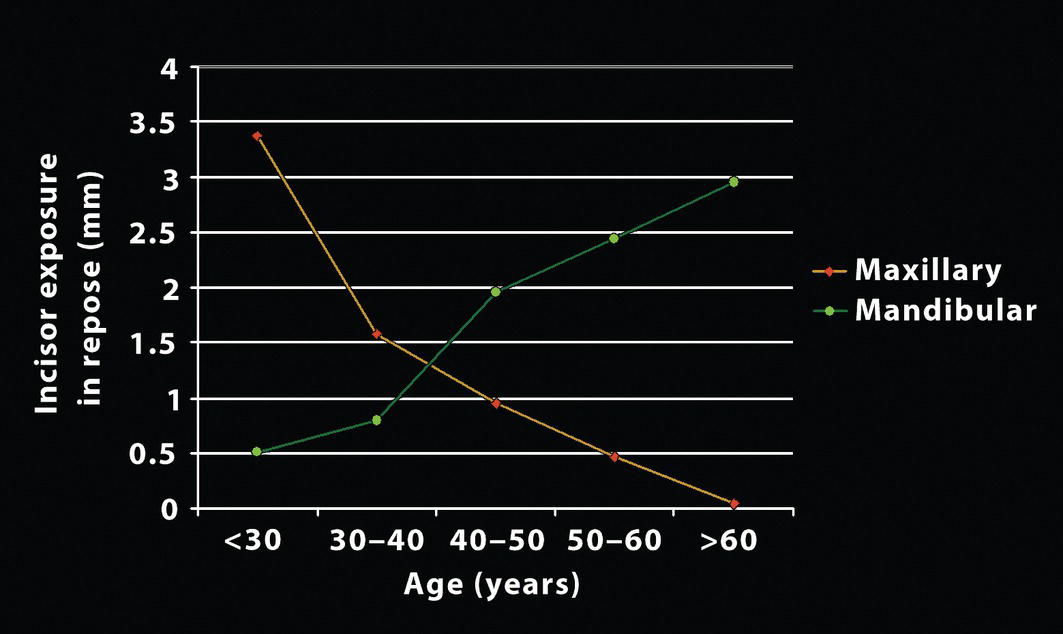
Vig and Brundo10 have provided normative mean values for incisor exposure in repose for Caucasian adults related to age (Table 23.2 and Figure 23.2):
The resting lower lip line may be defined as the vertical relationship between the superior border of the lower lip and the incisal edge of the maxillary incisor teeth. The lower lip should cover the incisal third of the maxillary central incisors.
In the animated state of smiling, the upper lip line should elevate to such a degree that the inferior upper lip border reaches the maxillary incisor gingival margin, displaying the entire incisor crowns, interdental papillae and up to 1–2 mm of gingivae.
Table 23.2Incisor exposure at rest relative to age
Figure 23.2 Line diagram illustrating changes in incisor exposure in relation to age – mandibular incisor exposure increases and maxillary incisor exposure decreases with age (see Table 23.2).
The resting and dynamic lip lines are also correlated with the type of malocclusion, with which a patient may present. For example, mandibular incisor exposure may be increased in Class III malocclusion (Figure 23.3A). Conversely, maxillary incisor exposure is often increased in Class II malocclusion, particularly if the maxillary incisors are excessively proclined (Figure 23.3B).
Upper lip–maxillary incisor relationship
Leonardo da Vinci described the importance of the ‘strongly movable section of the face around the mouth and chin in determining facial expression’, emphasizing the importance of observing the face in animation as well as in the static state.11 One of the most important facial aesthetic parameters is the degree of exposure of the maxillary incisor teeth in relation to the upper lip, both at rest and in animation, i.e. in speech and in smiling.12
Figure 23.3 (A) Increased mandibular incisor exposure in Class III malocclusion. (B) Increased maxillary incisor exposure in Class II malocclusion with proclined maxillary incisors.
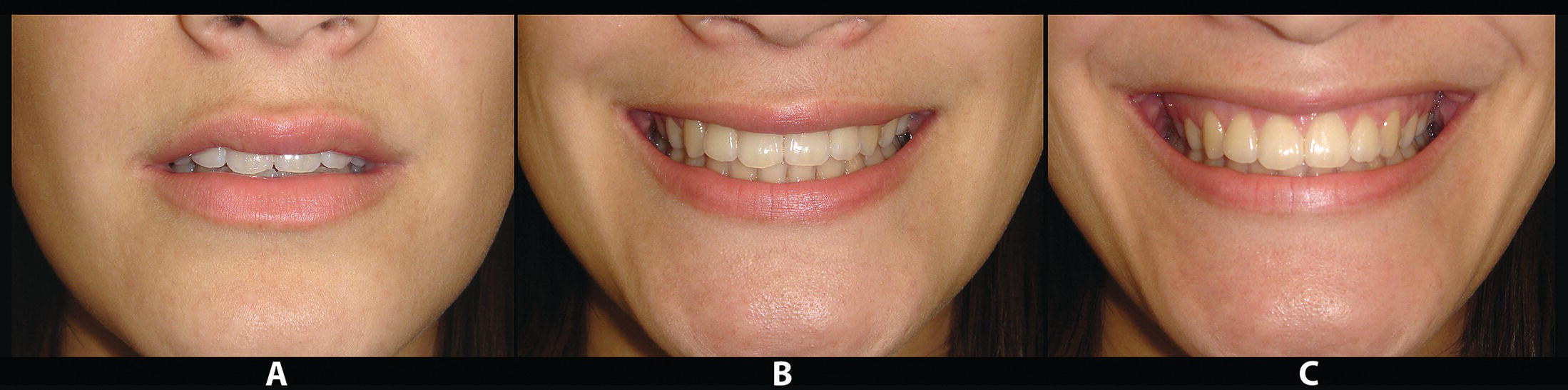
The vertical exposure of the maxillary incisors in relation to the upper lip at rest should be 2–5 mm, and on smiling the entire crown of the maxillary incisors should be exposed, with up to 1–2 mm of associated gingiva. A spontaneous smile, which is involuntary and expresses joyous emotion, tends to elevate the upper lip slightly more than a posed smile, which is voluntary (Figure 23.4).
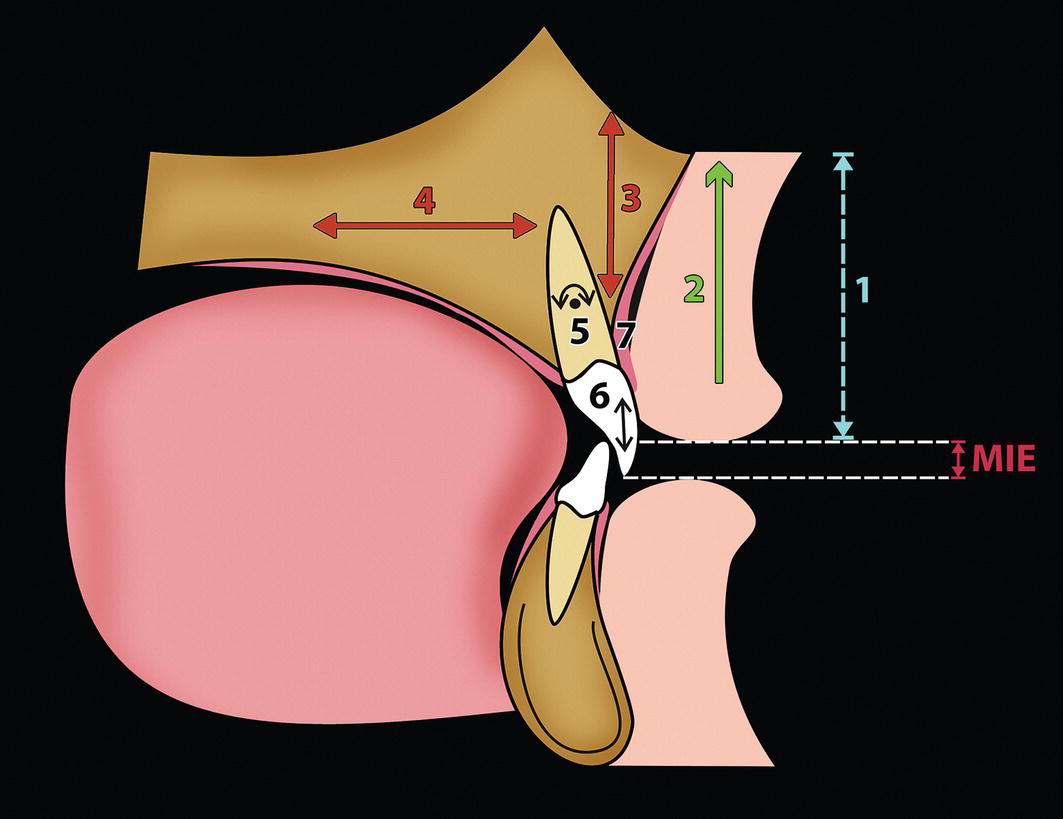
The ‘lip–incisor relationship’ depends on a number of factors (Figure 23.5), including12:
Upper lip height: Increased upper lip height will tend to reduce maxillary incisor exposure, and vice versa. Upper lip height, measured from subnasale (Sn) to stomion superius (Sts), is approximately 22 ± 2 mm in adult males and 20 ± 2 mm in adult females. Mid‐philtral height is roughly equal to, or 1–2 mm less than commissure height (measured from the oral commissure to a horizontal line through subnasale) (see Figure 17.21). Reduced mid‐philtral height results in an unattractive inverted arc appearance of the upper lip (see Figure 17.22); surgical procedures to increase the upper lip height may be required in such cases.
Figure 23.4 Upper lip–maxillary incisor relationship. (A) The vertical exposure of the maxillary incisors in relation to the upper lip is approximately 2–5 mm in repose. (B) With a posed smile the entire crown of the maxillary incisors should be exposed, with up to 1–2 mm of associated gingiva. (C) A spontaneous smile tends to elevate the upper lip more than a posed smile to a variable degree.
Figure 23.5 The ‘lip–incisor relationship’ and maxillary incisor exposure (MIE) depends on the following factors:
Upper lip height
Smile curtain – the muscular capacity to elevate the upper lip
Vertical position of the anterior maxilla and incisor teeth
Sagittal position of the anterior maxilla and incisor teeth
Inclination of the maxillary incisor teeth
Maxillary incisor crown height
Vertical level of the labial maxillary incisor gingival margins.
Smile curtain: The ‘smile curtain’ may be defined as the muscular capacity to elevate the upper lip. The elevation of the upper lip from repose to full smile exhibits considerable individual variability, averaging 7–8 mm (range 2–12 mm).14 If the position of the maxilla and maxillary incisors in relation to the face is correct, yet the patient presents with a ‘gummy smile’ due to vertical hypermobility of the upper lip, the option of botulinum toxin type A injections to the levator muscles of the upper lip is available. Alternatively, surgery to reduce the mobilization and elevation of the upper lip may be undertaken using the technique originally described by Kostianovsky and Rubinstein,15 later re‐described by Kamer16 (Figure 23.6).
Vertical position of the anterior maxilla and incisor teeth: The more inferior the position of the anterior maxilla, the greater the exposure of the maxillary incisors, and vice versa.
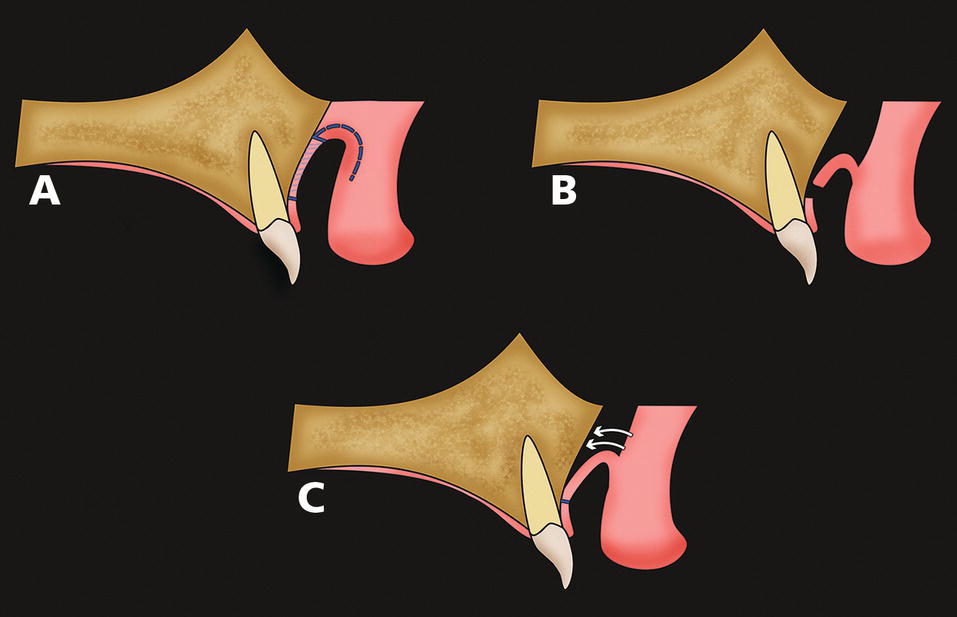
Figure 23.6 Kostianovsky and Rubinstein’s method of reducing upper lip mobilization when hypermobility of the upper lip is the primary aetiology of a ‘gummy smile’15: A horizontal strip of mucosa is excised from the labial surface of the alveolar mucosa, extending from the anterior alveolus region to the second molar region bilaterally. The upper border of the strip is the reflection of the upper labial sulcus and the lower border parallels it approximately 3 mm above the gingival margin. (A) The strip of mucosa is removed, leaving the periosteum intact. (B) A wide flap from the vestibular aspect of the upper lip is turned downward and sutured to the labial alveolar mucosa. (C) The surface between the alveolar periosteum and upper lip musculature is sealed; the resultant synechia reduces the elevation of the upper lip in animation.
Figure 23.7 Vertical maxillary excess (VME) – this case demonstrates total VME, with excessive exposure of the anterior and posterior maxillary dentition and associated gingivae, i.e. the ‘gummy smile’ extends posteriorly.
Sagittal position of the anterior maxilla and incisor teeth: The more anterior the position of the maxillary incisors, the greater the exposure of the maxillary incisors, and vice versa.
Figure 23.8 (A) Vertical maxillary excess; this patient demonstrated excessive gingival display at rest and on smiling. (B) Following superior repositioning of the maxilla (together with mandibular advancement to correct the Class II skeletal pattern), the incisor and gingival exposure has improved.
Figure 23.9 Anterior vertical maxillary excess (anterior VME) – this is due to excessive eruption of the maxillary incisor teeth and associated anterior gingivae, i.e. the ‘gummy smile’ is only evident anteriorly.
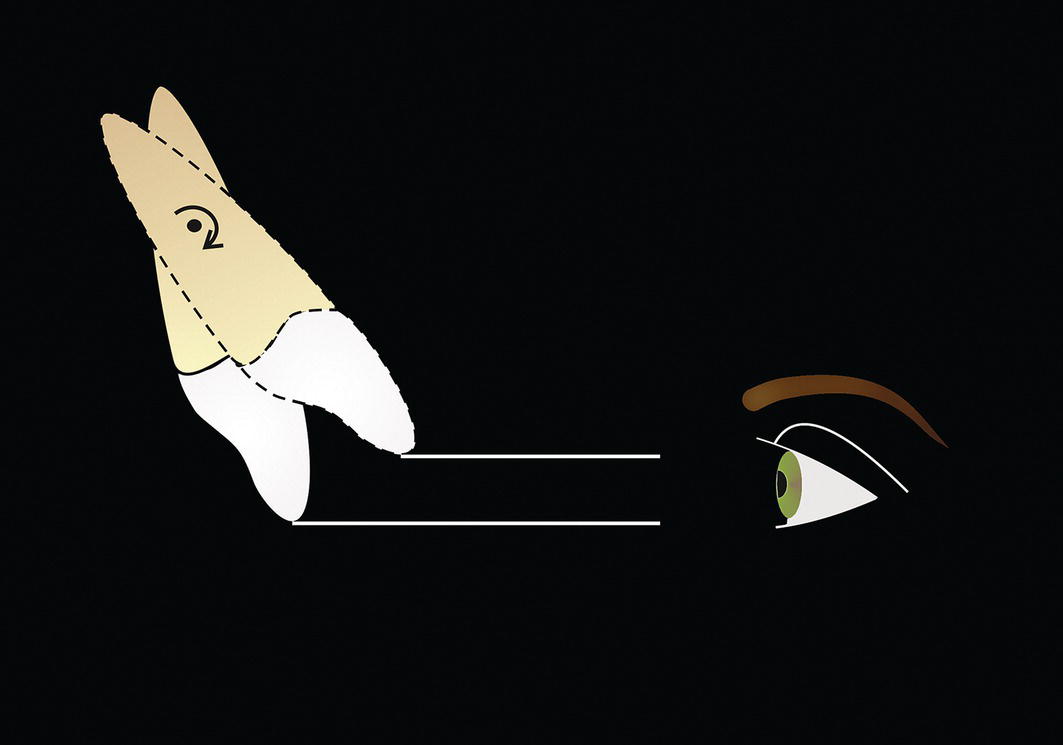
Inclination of the maxillary incisor teeth: Retroclination of proclined maxillary incisors towards the correct inclination increases the incisor exposure, as the teeth rotate around their centre of resistance (Figure 23.10). Maxillary incisor crown inclination may be ideally evaluated on a profile smiling view.
Maxillary incisor crown height, including the presence of incisal wear: Short maxillary incisor crowns and vertical wear of the incisor crowns reduces incisor exposure. Average maxillary central incisor crown height is approximately 10 mm.
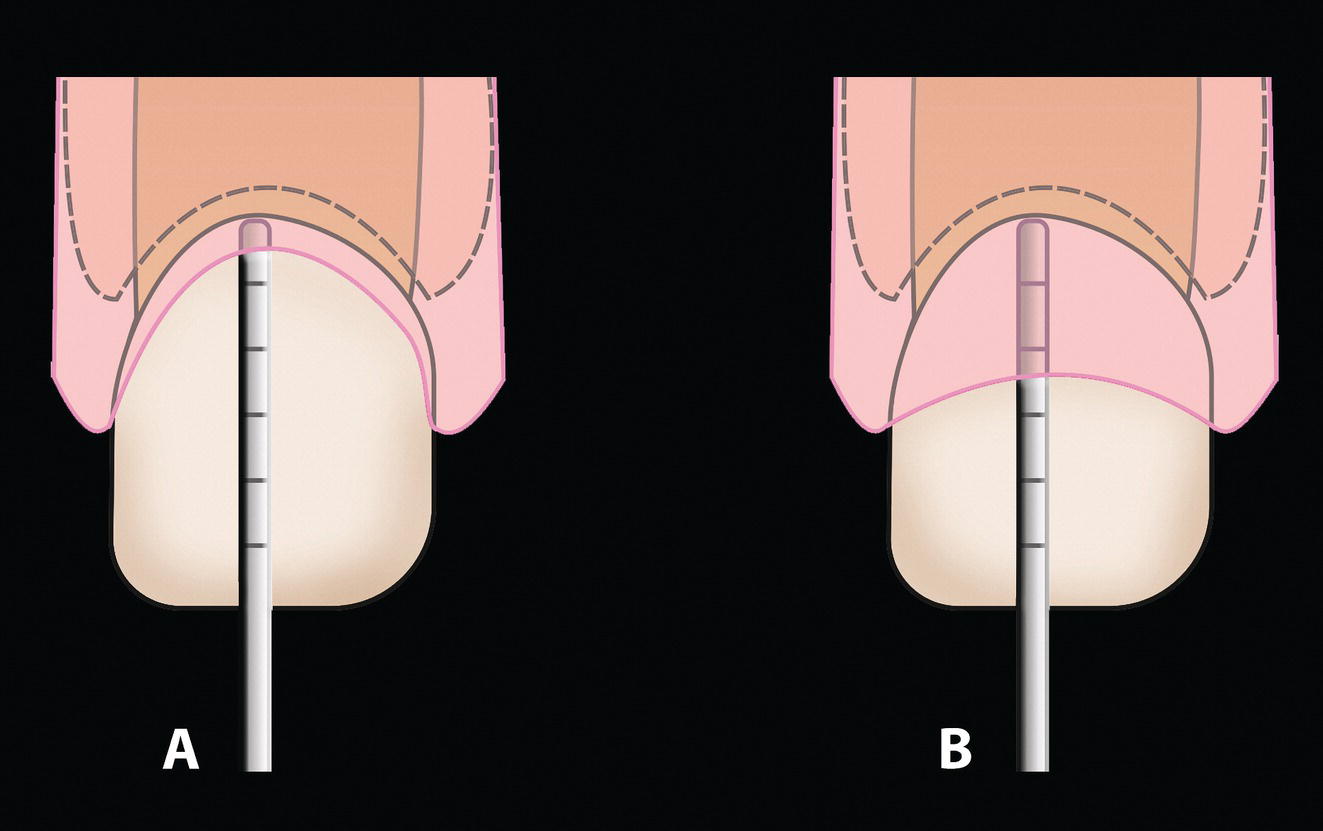
Vertical level of the gingival margins on the labial surface of the maxillary incisor crowns: It is important to note that the gingival margins of the maxillary incisors may migrate gingivally until late adolescence (described as delayed apical migration of the gingival margin), reducing gingival exposure and exposing the normal crown height. In adolescent patients with excessive gingival exposure, the gingival sulcular depth may be assessed with a periodontal probe. Normal sulcular depth is about 1 mm, with the cementoenamel junction located at the depth of the sulcus. If the sulcular depth is found to be significantly greater than 1 mm in the absence of gingival inflammation, it may take a number of years for the gingival margin to migrate to the normal relationship, i.e. the diagnosis is delayed apical migration (Figure 23.11). In such cases, gingivectomy may be required.17 Gingivectomy or crown lengthening procedures may also be required in adults with short clinical crowns and excessive gingival display.
Figure 23.10 Retroclination of proclined maxillary incisors towards the correct inclination increases the incisor exposure, as the teeth rotate around their centre of resistance.
Figure 23.11 Gingival sulcus depth may be measured by probing the sulcus with a periodontal probe on the labial aspect of the tooth. (A) Normal gingival sulcus depth is about 1 mm, with the cementoenamel junction located at the depth of the sulcus. (B) Sulcus depth significantly greater than 1 mm, in the absence of gingival inflammation, results from delayed apical migration; determination of the anatomical crown height specifies the amount of gingiva that may be removed.
Only gold members can continue reading. Log In or Register to continue