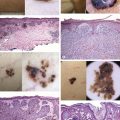
Histopathology:
Epidermal rete demarcating a lymphohistiocytic infiltrate in the superficial dermis
Histiocytoses
There are classic presentations of different histiocytoses (Fig. 10.2, Table 10.1), and the typical lesion is a dermal red–brown to pink papule for non-Langerhans cell histiocytoses. Such papules may also be seen in Langerhans cell histiocytosis (LCH), but the more common LCH lesion is an eroded and purpuric papule or plaque. In practice, there is significant overlap between various histiocytoses; the clinical distribution, other clinical lesions, and/or histopathologic features may be helpful in categorization.
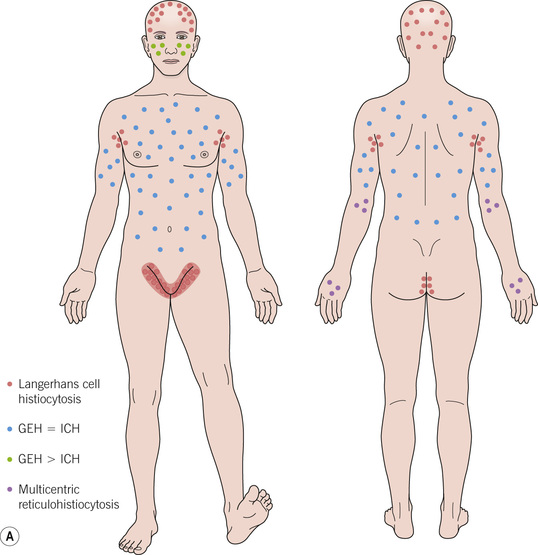
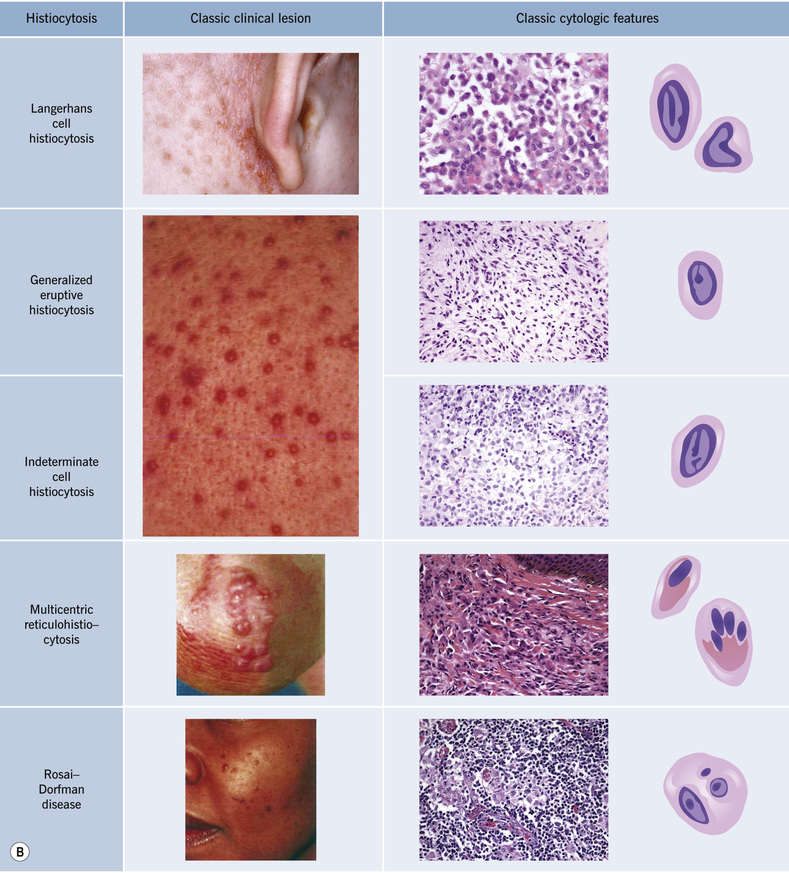
Fig. 10.2 Histiocytoses. A Typical distribution of different histocytoses. GEH, generalized eruptive histiocytosis; ICH, indeterminate cell histiocytosis. B Classic clinical lesion and cytologic features (“high magnification” view) of selected histiocytoses. Photographs courtesy, Irwin Braverman, MD; Ingo Haase, MD, and Iliana Tantcheva-Poor, MD; Jean L Bolognia, MD and Yale Dermatology Residents’ Slide Collection. From Bolognia JL, Jorizzo JL, Schaffer JV. Dermatology, 3e. London: Saunders, 2012, with permission.
Table 10.1
Classic features of selected histiocytoses
| Histiocytosis | Classic clinical features | Classic histopathologic features |
| Langerhans cell histiocytosis (Fig. 10.3A–C) | ||
| Generalized eruptive histiocytoma (Fig. 10.3D,E) | ||
| Indeterminate cell histiocytosis | ||
| Multicentric reticulohistiocytosis (Fig. 10.3F,G) | ||
| Rosai–Dorfman disease (Fig. 10.3H–K) | Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|