Pain, loss of motion, and instability in the small joints of the hand can result in debilitating loss of function and deformity. Salvage procedures are considered in the setting of complex nonreconstructable fractures, after failure of initial fracture treatment, and for the treatment of severe joint arthritides. This article reviews the merits of various reconstructive options in these settings and examines the pertinent anatomy, clinical challenges, and risk-benefit profiles of each option. The review is limited to salvage reconstructive procedures of the small joints of the hand.
Metacarpophalangeal joint reconstruction
Anatomy
The metacarpophalangeal joint (MCPJ) is a diarthrodial joint that is critical for functional hand motion and is based on an articulation of the head of the metacarpal and the proximal phalanx. The joint allows for extension, flexion, abduction, adduction, and rotational motion of the proximal phalanx. Extrinsic musculotendinous units and the intrinsic joint elements of capsule and collateral ligaments serve as joint stabilizers during key pinch and static loading.
The capsule of the joint is based on the composite structure of the flexor tendon sheath and the collateral ligaments. Along the volar capsule of the joint, the fibrous volar plate of the flexor sheath is firmly anchored to the base of the proximal phalanx with relatively weak attachments to the metacarpal head. This plate has an accordionlike or thatched structure that allows it to compress with the joint during motion, whereas its counterpart, the proximal interphalangeal joint (PIPJ) volar plate, is much more rigid. On the dorsal and lateral aspects of the joint exist longitudinal ridges that are in continuity with 2 pairs of stout collateral ligaments. The proper collateral ligaments (PCL) originate from the dorsal metacarpal head tubercle and insert along the volar lateral margin of the proximal phalangeal base. The accessory pair of collateral ligaments has a similar origin along the metacarpal tubercle but is more volarly inclined from its origin and inserts along the lateral margin of the volar plate.
Further differentiation of the collateral ligaments is based on the ulnar or radial basis of the PCL. These eccentrically oriented ligaments are the primary stabilizing force against joint dislocation in all 4 planes of movement. The radial collateral ligament is usually more clinically relevant because it is responsible for stability of the finger during pinch and grasp functions.
Unique to the MCPJ is the so-called cam effect created by the nonspherical shape of the metacarpal head. The distance from the axis of rotation of the metacarpal head to the base of the proximal phalanx is greater for flexion than extension. As the MCPJ is brought out of flexion, the collateral ligaments shorten to maintain joint stability by dynamically changing ligamentous length relative to the fixed joint axis. This intrinsic compensatory ability may explain the pathophysiology of MCPJ stiffness and decreased range of flexion after joint trauma or prolonged immobilization in MCPJ extension. Inflammation and decreased motion may decrease the elastic potential of the collateral ligaments, thereby restricting motion that requires a lengthening of the ligaments, such as during active flexion. For this reason, prolonged immobilization and splinting of the hand with the MCPJs in flexion provide a greater chance of return of motion compared with a posture of extension.
MCPJ Arthrosis
Although traumatic indications and late sequelae of osteoarthritis (OA) may account for many of the indications for joint reconstruction, systemic arthridities, such as rheumatoid arthritis, also deserve special consideration. Unlike traumatic or idiopathic OA, which is usually asymmetric and joint specific, rheumatoid arthritis is a systemic disease that affects multiple joints of the hand in a diffuse manner.
The pathophysiology of the disorder involves an overgrowth of the joint synovium causing secondary deformities with articular destruction and loss of normal soft tissue architecture. The MCPJ develops a posture of volar subluxation, ulnar deviation, and slight pronation. The extensor tendon migrates ulnarly and volarly in relation to the metacarpal head, and active extension, followed by passive extension, is ultimately lost. This migration in turn creates tendon imbalance in the distal digit and may be seen in conjunction with boutonniere or swan neck deformities.
Rheumatoid disease of the hand is a continuous process. Despite severe disease, the hand may still be quite functional for the patient. The residual function is dependent on a delicate balance of the musculotendinous units. As a result, a cosmetic deformity may be a poor indication for intervention and may incur the risk of only worsening function. The alleviation of pain and functional stability should be the primary indicators for surgery in the rheumatoid hand. The perioperative considerations of impaired immune function, wound healing, and the tendency for disease recurrence must always be considered. Because reconstructive options, including arthroplasty and arthrodesis, are frequently dependent on adequate bone stock and healing, the rates of fracture, nonunion, and malunion may be significantly increased, and both the patient and the provider should be prepared for such outcomes.
MCPJ Arthrodesis
Frequently, hand and finger function is not simply limited by a lack of range of motion or strength but by debilitating pain. In the patient in whom active or passive range of motion is limited, arthrodesis may offer the practitioner and the patient an opportunity to markedly reduce the symptoms of a painful joint.
Fusion of the MCPJ can also be applied in other clinical settings. In the laborer with traumatic arthritis, fusion may create a functional grip. By determining the angle that best provides apowerful or stable grip, such as during grasp of a specific tool or instrument, the patient may enjoy a functional reconstruction with a short recovery period. Index finger MCPJ arthrodeses are generally recommended to be performed in approximately 25° flexion. Fusion angles of other digits are planned with a slight cascade of increasing flexion moving ulnarward, which is typically at an increase of about 5° flexion in each successive ulnar adjacent digit.
Consideration is given to arthrodesis if the benefits of pain relief and stability outweigh the cost of loss of motion. The selection between motion-sparing and motion-eliminating salvage procedures is different for each digit. In digits 2 through 5, the MCPJ contributes significantly to total arch of motion (TAM) of the digit. A loss of this motion changes the function of the hand dramatically from baseline. Alternatively, the thumb MCPJ often provides little contribution to the thumb TAM, and arthrodesis at this site is well tolerated. Furthermore, because the hand is a dynamic construct with different needs at the MCPJ between the small to index finger, the fusion of a joint that has increased coronal forces or a tendency toward subluxation, such as the index MCPJ during key or pinch grasp, may be a more stable alternative.
The techniques commonly used for arthrodesis of the MCPJ include plate fixation, Kirschner wire (K-wire) fixation, tension band wiring, and screw fixation.
MCPJ Silicone Implant Arthroplasty
Silicone implant arthroplasty uses a 1-part constrained device for MCPJ reconstruction. The constrained nature of the device allows it to be used in settings of severe ligamentous and articular surface destruction. The rheumatoid joint is an excellent example of the type of pathologic condition in which a constrained device may provide benefit because the surrounding capsular structures may be lax or may require reconstruction, and soft tissues are often inadequate or unable to provide joint stability independently. The 1-piece flexible-hinge design of the device was originally created and popularized by Swanson and is under maximal stress during flexion. His initial results held promise of the use of this implant to serve as a spacer for the development of stability through encapsulation. Multiple studies have continued to show favorable early results but with a possible decline in outcomes after long-term review.
Olsen and colleagues (1994) provided 7-year follow-up data on 60 silicone implant arthroplasties performed in 16 patients with rheumatoid arthritis. The investigators noted continued improvement of passive motion years after surgery but limited active motion (30°) despite longer follow-up. They also noted a high incidence of continued pain (8/16 patients) multiple years after arthroplasty, and only 9 of 16 patients reported satisfaction with their reconstruction.
Kirschenbaum and colleagues provided 8.5-year follow-up data on 27 patients with rheumatoid arthritis with 144 MCPJ silicone implant arthroplasties. The investigators reported stable improvement of ulnar deviation and extension deficit. Although fracturing of 15 of the implants was noted, no patients reported pain at long-term follow-up, and all patients were satisfied with their arthroplasties. Alternatively, Blair and colleagues reported limited improvement in the flexion-extension arc of motion in a longer-term follow-up (54 months average) as compared with preoperative motion (17° increase overall). The investigators also noted a frequent decline of ulnar deviation to preoperative values.
Bieber and colleagues compared the initial postoperative motion of MCPJ silicone implant arthroplasties with a follow-up average longer than 5 years. Their study demonstrated that the ulnar deviation, extension deficit, and total arc of motion again deteriorated at long-term follow-up.
An even longer-term retrospective review of 1336 implants in 381 patients undergoing metacarpophalangeal silicone joint arthroplasty for rheumatoid arthritis was performed by Trail and colleagues. The investigators sought to assess the rate of implant failure and need for revision surgery. Using Kaplan-Meier survival curves based on the terminal events of implant loosening or revision, a total of 1336 implants were identified with 83% survival of the implant at 10 years, and 63% at 17 years. Although the revision rate was very low, the rates of fracture or displacement of the implants was significantly higher (42% at 10 years, 66% at 17 years). This finding indicated that implant failure did not prohibit the construct from serving as a good long-term functional reconstruction. Although the scar tissue surrounding the implant is believed to impart some stability, the study by Trail and colleagues noted that additional soft tissue rebalancing procedures correlated with increased survivorship of the implant.
Less enthusiastic results were reported by Goldfarb and Stern, who reviewed their long-term outcomes of 208 MCPJ silicone arthroplasties at an average follow-up period of 14 years. The investigator’s early results demonstrated an improvement in extension and ulnar drift, but they noted an overall decline in function and position over time. The average initial arc of motion improved from 30° to 46° postoperatively but returned to 36° at the time of follow-up. Extension deficit and ulnar drift also improved postoperatively but diminished at long-term follow-up. In terms of implant survival, 63% were broken and another 22% were deformed at the time of final follow-up. Similarly, pain-free motion was seen in only 27% of the hands, and 38% of patients expressed satisfaction with their hand function.
The use of silicone arthroplasty in the MCPJ has been most widely studied in the rheumatoid population. The initial encouraging results observed with its use have been demonstrated to diminish with longer-term follow-up. Because the enthusiasm for MCPJ arthroplasty in this population has waned, the need for surgical reconstruction has also diminished with the advent of increasingly effective methods of medical management for rheumatoid arthritis. Although much less frequently performed than decades past, silicone implant arthroplasty has remained the standard offering for surgical reconstruction when required.
MCPJ Pyrolytic Carbon Arthroplasty
In an effort to overcome some of the problems associated with silicone arthroplasty, such as implant pistoning, bone and/or implant fracture, and recurrent deformity, efforts have been directed at the creation of a device that might better mimic normal joint kinematics. The pyrolytic carbon arthroplasty device attempts to mimic the normal motion seen in the joint, but its nonconstrained 2-part design must rely on surrounding soft tissue constraints to provide joint stability.
The implant is a synthetic construct engineered from the pyrolysis of hydrocarbon gas, and it achieves an elastic modulus similar to that of cortical bone. This property may allow it to better share loading forces with the proximal and distal cortical bone for implant-bone stress transfer and decrease implant failure, fracture, or wear. In a retrospective review performed by Cook and colleagues, long-term follow-up and functional status of 151 metacarpophalangeal pyrolytic carbon arthroplasties were assessed. Most of these implants were performed for rheumatoid arthritis. At an average follow-up of 11.7 years, the investigators identified a statistically significant increase in the arc of motion from 39° preoperatively to 52° after arthroplasty. In addition, the arc of motion achieved was in a more extended posture (an average of 16° greater extension), resulting in an increasingly functional and extended finger. Survivorship analysis identified an annual failure rate of approximately 2.1% and a 10-year survival rate of 81.4%. Also, radiographic changes indicative of periprosthetic bone lucency and bone erosion were approximately 23% for pyrolytic carbon implants compared with 87% for silicone constrained implants, as reported by Derkash and colleagues. About 82% of implants maintained their original postoperative reduced position. Of 151 implants, 18 necessitated revision due to various reasons, including stiffness, malpositioning of the components, loosening, implant fracture, subluxation, and dislocation.
In a similar analysis, Parker and colleagues reviewed their experience with 142 consecutive arthroplasties using a newer-generation pyrolytic carbon implant in the MCPJ for both OA and rheumatoid arthritis with an average follow-up of only 17 months. Early gains in the arc of motion after implant placement were seen in both groups of patients. Preoperative arc of motion in the OA group improved from 44° to 58° at 1 year, and the rheumatoid arthritis group experienced gains from 32° to 45° in total motion. However, although radiographs demonstrated stable implants in all patients with OA, the rheumatoid arthritis group had a markedly increased rate of axial subsidence and periprosthetic erosions, at 10.5% and 16.4% of joints, respectively. In addition, in those patients with rheumatoid arthritis with more than a year of follow-up, the rate of axial subsidence continued to increase to 55%, and 45% of implants demonstrated periprosthetic erosions.
The pyrolytic carbon joint arthroplasty may offer a durable and biomechanically stable option for joint reconstruction in the patient with modest deformity, whereby joint stability and soft tissue constraints are not markedly compromised. However, given the recent data on short-term follow-up of the newer-generation design, with increasing rates of subsidence, periprosthetic fracture, and joint instability, the pyrolytic carbon implant may suffer from similar long-term deforming sequelae as the silicone implant, especially in the patient with rheumatoid arthritis.
Vascularized Joint Transfer MCPJ Reconstruction
The loss of joint congruity and cartilage integrity after acute injury or chronic attrition of the MCPJ can lead to a painful and stiff finger. Arthrodesis offers reliable pain relief at the cost of motion. Implant arthroplasty offers pain relief with motion preservation with a risk of instability and limited longevity. The concept of autologous vascularized joint transfer could theoretically provide pain relief with lasting stability and motion preservation. Vascularized joint transfer may also provide a ligamentous and tendon/soft tissue reconstruction alternative in addition to the arthroplasty component.
Initially described as a nonmicrosurgical procedure, the PIPJ or metatarsophalangeal joint (MTPJ) of the toe was harvested as an avascular graft and used in the total joint arthroplasty of the MCPJ. The nonvascularized nature of these grafts resulted in cancellous and cartilaginous resorption during the early phase of healing and ultimately the collapse of the construct.
Later described by Bunke and colleagues in 1967, vascularized joint transfer may avoid the issues of chronic avascular collapse and synovial degeneration. Modified by Foucher and others, the vascularized joint transfer is usually obtained from either the PIPJ or the MTPJ of the toe. The donor toe joint defect is usually arthrodesed with a bone graft.
Although the procedure has demonstrated a reliable means of providing stabile reconstruction and pain relief, the results in motion preservation have been disappointing. Regardless of use of the MTPJ or PIPJ of the toe as a donor site, the resultant range of motion for digital MCPJ reconstruction in the hand is limited to approximately 30°. The greatest advantage of vascularized joint transfer may exist in treatment of the pediatric trauma patient. The MTPJ, as in the analogous hand joint, has an epiphyseal growth plate at the proximal and distal borders of the joint. These growth plates are in the metatarsal and proximal phalangeal bones, respectively. If the joint is harvested with these growth plates, some continuation of bony growth may be demonstrated in the graft after the joint transfer. Therefore, in pediatric patients with joint damage, including those with epiphyseal damage, joint transfer may offer a reconstructive option that maintains some joint motion and stability and an appropriate anatomic growth potential.
In addition, using the concept of “spare parts” surgery in the setting of multiple digital amputations or crush injuries, the reconstruction of the most functional finger and MCPJ may be aided by using a heterodigital transfer of a vascularized joint from a digit that would otherwise not be saved.
Proximal interphalangeal joint reconstruction
PIPJ Pathology
As with any hand injury, trauma can result in a wide variety of injuries that can affect the PIPJ. Specifically, bony and soft tissue destruction can cause the joint to become unstable, while extended immobilization can contribute to joint stiffness. Bony destruction can range from simple fracture dislocation to total bone loss, whereas soft tissue destruction includes joint capsule disruption or volar plate avulsion leading to instability. The effects of trauma may require immediate joint reconstruction techniques if the fracture is not amenable to conventional reduction and fixation procedures, or delayed reconstruction may be required to address posttraumatic OA.
In addition to these mechanical derangements, chronic joint pain can be the predisposing factor to joint reconstruction. Chronic pain can be a result of idiopathic OA or inflammatory arthritis. As with most treatments, the cause of joint destruction guides the modality of reconstruction.
PIPJ Anatomy
The PIPJ is configured to permit a large range of flexion and extension with limited radial or ulnar deviation. The stability of this joint is achieved via a combination of the bony architecture and the joint capsule. Because of this configuration, approximately 100° motion is capable at the joint. Despite the similarities in function of the 2 joints, the anatomy of the PIPJ differs from that of the MCPJ in distinct ways.
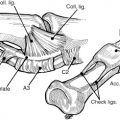
Unlike the MCPJ, in which the metacarpal has a cam shape with a volar flare, the proximal phalanx has a bicondylar circular head. The lack of volar flare permits a uniform tension on the collateral ligaments throughout joint motion. However, similar to the MCPJ, the collateral ligaments are composed of both PCL and accessory collateral ligaments (ACLs). Both originate from the condylar recess of the proximal phalanx, with the larger PCL inserting into the volar third of the middle phalanx and the volar plate. The more proximally located ACLs run in a more volar direction and insert onto the volar plate only.
The volar plate of the PIPJ differs from that of the MCPJ. The distal insertion is the strongest, particularly at the lateral margins where the ACLs insert. Paired extensions, called checkreins, extend proximally and insert onto the proximal phalanx at the level of the A2 pulley. These structures limit hyperextension of the PIPJ and provide a strong volar stabilizing force. The PIPJ volar plate does not contract with flexion as the metacarpophalangeal volar plate does but instead slides with finger movement for increased stability during axial loading.
PIPJ Implant Arthroplasty
The primary indication for PIPJ implant arthroplasty is pain from idiopathic and posttraumatic arthritis or inflammatory arthritis. Although this condition provides a motion-sparing option for joint reconstruction, patients primarily seeking improvement in range of motion should be cautioned. Patients with active infection or poor soft tissue coverage or those who have lost the use of the extensor or flexor function are also poor candidates.
Implant composition has undergone numerous changes and evolved since the first description 70 years ago. Currently, 2 frequently used options for PIPJ implant arthroplasty are constrained flexible silicone implants and nonconstrained surface replacement arthroplasty (SRA) options.
Flexible silicone elastomer implants, unlike their hinged predecessors, are implanted as a single spacer. The implant has flexible tapered intramedullary stems that provide stability and a fulcrum for flexion and extension. Lin and colleagues reviewed 69 silicone arthroplasties at an average of 3.4 years of follow-up. The cohort included a heterogeneous group of patients with OA and inflammatory arthritis. The investigators found no significant improvement in motion, but pain relief was achieved in 66 of 69 joints. Ashworth and colleagues followed up 99 proximal interphalangeal (PIP) silicone implant arthroplasties in rheumatoid arthritis cases for an average of 5.8 years. The investigators noted very good pain relief but a loss in average range of motion from 38° preoperatively to 29° postoperatively. These findings were echoed by Takigawa and colleagues in a 2004 study of 70 silicone PIP arthroplasties for an average follow-up period of 6.5 years. This cohort also included a variety of patients with OA and inflammatory arthritis. Although pain relief was very good, there was no significant change for range of motion in postoperative compared with preoperative examinations.
SRA is an alternative to silicone spacers. Similar to other joints, including the MCPJ of the hand, PIP SRA attempts to re-create the normal anatomic geometry of the joint. This arthroplasty uses 2 implants, one that replaces the proximal joint surface and another distal component that allows the implants to articulate. These 2-piece nonhinged implants rely on collateral ligament integrity to maintain PIPJ stability. The first PIPJ SRA was described in the 1990s and includes a chromium-cobalt alloy proximal component and an ultra-high–molecular weight polyethylene distal component. A second type of SRA, made of pyrolytic carbon, is also available. When compared with silicone arthroplasty, SRA has been shown to have analogous results. Particularly with the metal on polyethylene SRA, multiple studies have shown improvement in arc of motion and pain relief.
Regardless of implant type, the surgical technique is similar. Volar, dorsal, or lateral approaches may be used, although it has been suggested that better results may be achievable with dorsal access. Osteotomies are made to remove the subchondral base of the middle phalanx and head of the proximal phalanx, taking care to preserve the attachments of the collateral ligaments, particularly with SRA. Implants are chosen after appropriate trials have been selected and inserted in place, confirming adequate motion of the joint.
Regardless of technique or implant material, the range of motion of the PIPJ after arthroplasty is considerably less than an unaffected joint. In 2008, Squitieri and Chung reported the outcomes of their systematic review of finger joint replacement. The investigators found that the mean arc of PIPJ motion for silicone and pyrocarbon (pyrolytic carbon) implants was 44° ± 11° and 43° ± 11°, respectively, with the pyrocarbon group having a considerably higher complication rate. Overall the outcomes for pyrolytic carbon SRA have been varied. Most of the literature indicates that although pyrocarbon arthroplasty may be helpful in reducing pain, there is minimal, if any, improvement in the range of motion of the joint. Nunley and colleagues studied posttraumatic OA PIPJs treated with pyrocarbon implant arthroplasty. At 1-year follow-up, the investigators noted no significant pain relief and loss of motion averaging 10°. These results led the investigators to abandon the implant use and the study protocol. Tuttle and Stern studied 18 pyrocarbon implant arthroplasties in OA joints followed up for 13 months. The investigators noted good pain relief but no improvement in range of motion and a high complication rate. Bravo and colleagues examined 50 PIP pyrocarbon implants at an average of 27-month follow-up in a heterogeneous group of patients with inflammatory, idiopathic, and posttraumatic OA. Pain relief was satisfactory; however, range of motion improved only 7° and the rate of secondary operations was 28%, with 8% patients requiring revision arthroplasty because of complications. Sweets and Stern reported very disappointing results in a 5-year follow-up study of 31 pyrocarbon PIP implant arthroplasties in patients with OA, noting an eventual loss of motion from 56° preoperatively to 28° at longer-term follow-up. Complications were frequent, and patient satisfaction was variable.
It seems that PIP pyrocarbon implant arthroplasty excels greatest for pain relief. This arthroplasty does not provide improvement in range of motion and may be accompanied by a high rate of complications. Complications include joint squeaking, subsidence, dislocation, and need for revision. Given these limitations, as well as the technical demands of the procedure and relative material cost, the role of these implants may be limited.
PIP Arthrodesis
Indications for PIP arthrodesis are the same as for other reconstructions, with pain and joint instability being the most pertinent. This indication includes severe arthritic pain that limits function at sites where arthroplasty is not an option or has failed or is precluded by joint instability. Arthrodesis can be very successful at relieving pain while still providing the patient with a finger that maintains length and can be functional. For the ulnar digits, fusion may be more unfavorable because it can negatively affect grip strength, and the finger frequently gets caught up in pockets or tight spaces. However, for the more radial digits, particularly the index finger, fusion may provide the patient with a stable digit with effective key pinch.
As arthrodesis is often the last option before amputation, a significant discussion with the patient must take place before surgery. It can be helpful to temporarily splint the joint or immobilize it with a K-wire before surgery so that patients can experience how their hand will function with a stable motionless joint. As with the MCPJ, the amount of flexion for each finger may vary, and this should be adjusted to fit with the patient’s needs. Typically the amount of flexion increases from the radial to the ulnar digits, with the index finger being placed in 40° of flexion, 45° for the middle finger, 50° for the ring finger, and 55° for the small finger.
Although there are several techniques for PIP arthrodesis, there are basic components that each must accomplish. Key points may include a dorsal approach that preserves the extensor mechanism and joint capsule to close over hardware. To achieve bony fusion, the articular cartilage must be removed from the proximal and middle phalanx before hardware fixation. This removal can be done in either a cup and cone manner to allow adjustments of the fusion before hardware fixation or an angled resection. Once accomplished, the joint is immobilized until bony fusion occurs (about 6–8 weeks). Frequently used techniques include
K-wire fixation
A combination of multiple crossing K-wires are used to obtain stability at the desired angle and rotation. This type of arthrodesis is the simplest in technique, with comparable rates of nonunion and malunion but higher complication rates.
90–90 interosseous wiring
This technique uses 2 perpendicular steel wire loops.
Tension band wiring
Tension band wiring includes 2 parallel K-wires across the arthrodesis site with a transversely placed interosseous wire through the base of the middle phalanx progressing proximally in a figure-of-eight model along the dorsal cortex of the proximal phalanx. This wiring works to counteract the forces of the flexor tendons and causes compression at the volar surface of the arthrodesis.
Plate fixation
This technique uses a single plate along the dorsal cortex and bent to the desired angle.
Compression screws
In this method, a lag or headless screw is fixed in an axial orientation. This technique is shown to have favorable success compared with other methods of fixation, with the main drawback being the palpability of the screw head; however, this is reduced with the headless screws. This technique is more difficult in arthrodeses performed in significant flexion and is often reserved for extended interphalangeal fusions (ie, distal interphalangeal [DIP] joint arthrodesis).
Volar Plate Arthroplasty
Fracture dislocations of the PIPJ can be unstable if the osseous support of the volar lip of the base of the proximal phalanx is significantly compromised. This instability is directly proportional to the percentage of volar base of the middle phalanx fractured. If less than 20% of the articular surface of the middle phalanx is involved, the joint is typically stable. If 30% to 50% is involved, the joint is tenuous, and greater than 50% is unstable. If the fragments are large enough to permit restoration of architecture through bony fixation, fracture management options are used. If the fragments are highly comminuted and affected and preclude joint restoration, salvage options are considered to achieve joint congruity and stability.
Volar plate arthroplasty (VPA) uses the volar plate to reconstruct the volar joint surface of the middle phalanx and restore joint congruity in these larger nonreconstructible comminuted fractures. This technique can be performed acutely or in a delayed manner.
For exploration and repair, the joint is exposed via a volar approach and hyperextended after release of the collateral ligaments. After removal of comminuted fragments, the volar plate is released from the collateral ligaments and mobilized distally into the defect in the middle phalanx. The plate is then secured with a suture anchor or pullout wire or suture through the middle phalanx. The joint is temporarily stabilized in slight flexion with K-wire fixation for approximately 3 weeks.
Reported outcomes for VPA are satisfactory with better results obtained when surgery is performed in the acute period. In a review of patients with at least 10 years of follow-up after VPA, the average range of motion was 95° when performed within 6 weeks, compared with 78° when performed after 6 weeks. The same senior investigator reviewed results from patients with an average of 11.5 years of follow-up and found that those patients treated within 4 weeks attained a range of motion of 85°, whereas those receiving arthroplasty after 4 weeks achieved a motion of 61°.
In addition, there have been reports of VPA to treat OA of the PIPJ. Although the investigators did not show a difference in range of motion or grip strength, all patients had significant reduction in pain symptoms.
Osteochondral Autografting
Hemihamate arthroplasty provides a reconstructive option for PIP dorsal fracture dislocations in which 50% or more of the articular surface is involved and cannot be restored. This technique involves using a hemihamate osteochondral autograft to reconstruct the base for the middle phalanx and was first described in 1999. The technique can be used acutely or as a salvage procedure. Use of the hamate fragment with articular cartilage attempts to re-create the joint surface of the middle phalanx to restore joint function. This re-creation is possible because of the similarity between the distal dorsal aspect of the hamate and the proximal volar portion of the middle phalanx. The sagittal ridge of the articular surface of the hamate that divides the cartilage contacting the fourth and fifth metacarpals is used to mimic the interfossal ridge of the proximal phalangeal base, which divides the ulnar and radial fossae, respectively.
To determine the amount of hamate required for reconstruction, the PIPJ must first be examined. This examination is done through a volar approach, hyperextending the joint to expose the volar surface of the middle phalanx. Once it is confirmed that the base of the middle phalanx is not suitable for internal fixation, the size of hamate required for reconstruction can be estimated in 3 dimensions. The hamate autograft is harvested via a dorsal approach exposing the distal articular surface with the central ridge between the ring and small finger. Two sagittal (longitudinal) cuts determine the length, whereas the axial (transverse) cut determines the width. The coronal cut through the distal surface of the hamate, which is the most difficult, corresponds to the volar-dorsal dimensions of the fragment. The graft is fixed into place with interfragmentary screws and contoured appropriately. The joint is then reduced, stability is confirmed, and the volar plate and soft tissues are repaired.
Retrospective studies evaluating this technique have shown positive outcomes in both acute and chronic PIP fracture dislocations. After hemihamate reconstruction, active PIP motion ranges from 70° to 85° with low pain and Disabilities of the Arm, Shoulder, and Hand scores and comparable grip strength to the contralateral hand.
Other donor sites for osteochondral autografting have been described for reconstruction of small joints of the hand, including the opposing surfaces of the second and third carpometacarpal joints, MTPJ, and osteochondral segments of ribs. The hemihamate reconstruction has become the most widely used and studied technique for replacement of the base of the proximal phalanx.
For injuries related to the condyles of the proximal phalanx, perhaps the most promising innovation was recently described by Cavadas and colleagues. This team performed cadaveric evaluation of the similarities of the ulnar base of the small finger metacarpal with the proximal phalangeal condyles. The investigators demonstrated a similar shape but a greater arc of curvature of 40% to 50% of the donor surface than the PIP condyles. Despite this anatomic discrepancy, the team reported on a clinical series of 16 unicondylar osteochondral reconstructions using this technique with a 4.8-year average follow-up. An average of 49° active motion was achieved in these difficult cases. This finding suggests that this technique may serve as a useful tool in the setting of unicondylar bone loss of the PIPJ.
Vascularized Joint Transfer for PIPJ Reconstruction
Vascularized PIPJ reconstruction involves the transfer of an autologous joint, either from a toe or another finger to reconstruct the PIPJ. The indications mentioned earlier for joint transfer reconstruction of the MCPJ are also applicable to the PIPJ. The pertinent clinical difference in consideration of vascularized joint transfer for PIPJs is the important contribution of the PIPJ to the digits’ total active motion. Achieving minimal motion with such a transfer may be functionally more acceptable at the MCPJ than the PIPJ. Although the studies are limited, it seems that the average range of motion achieved in PIPJ reconstruction (24°) is even less than is achieved in MCPJ reconstruction (32°–34°) using toe joints as donors.
After multiple digital amputations or trauma, a finger joint can be used for transfer from a nonsalvaged digit. In this case, a double osteotomy is performed to isolate the donor joint, with care taken to preserve the volar plate and digital vessels. The recipient site is prepared with extensor tendon preparation and bone cuts, ideally preserving the flexor sheath. The donor joint is inset with bone stabilization via K-wires or interosseous wiring. The flexor tendon sheath is reattached to the donor volar plate, and the extensor tendons are secured by separating into 2 slips, one secured to the central slip and the other to a lateral band.
Heterodigital joint transfers can be performed in the setting of multidigital trauma. Joints from otherwise nonsalvageable digits may be used as pedicled or free microvascular transfers.
If the donor joint is from the same finger, the transfer is termed homodigital DIP to PIP transfer. In this instance, the DIP joint is transferred proximally on its digital pedicle to reconstruct the PIPJ. The finger becomes a 2-joint system but gains motion as the PIP contributes more to the arc of the finger than the DIP.
Reports on outcomes for vascularized joint transfers are few. One study compared the different types of joint transfer performed in 26 patients. These included heterodigital island, homodigital island, free heterodigital, and second toe transfers. The mean active range of motion was 56° for heterodigital island, 52° in the homodigital island, greater than 65° in the free heterodigital island, and only 33° in the second toe transfers. All had significant extension lag ranging from a mean of 21° to 39°. In a series of 11 second toe to PIPJ transfers, the investigators found an average range of motion of 47°, with 41° extensor lag at a mean follow-up of 15 years.
Restoration of stability, resolution of pain, and preservation of motion are ideal goals in the setting of secondary small joint reconstruction of the hand. The surgeon must be familiar with the relative benefits of each of these options and the specific demands of the diseased joint to maximize results and function.
The authors have nothing to disclose.
Related posts:
 Free Functional Muscle Transfer for the Upper Extremity
Free Functional Muscle Transfer for the Upper Extremity
 Scar Contractures of the Hand
Scar Contractures of the Hand
 Functional Reconstruction of the Hand: The Stiff Joint
Functional Reconstruction of the Hand: The Stiff Joint
 Current Status of Brachial Plexus Reconstruction: Restoration of Hand Function
Current Status of Brachial Plexus Reconstruction: Restoration of Hand Function
 Treatment of Nonunion and Malunion Following Hand Fractures
Treatment of Nonunion and Malunion Following Hand Fractures
 Thumb Reconstruction
Thumb Reconstruction
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


