Aging skin is among the most common patient concerns in a facial plastic surgery practice. Ultraviolet (UV)-induced damage expedites the pace of intrinsic aging, resulting in many of the visible signs of aging, such as rough skin texture, pigmentation irregularities, fine and deep wrinkling, and inelasticity. Primary prevention of UV and environmental damage with proper skin care and the use of sunscreen are critical. There is great interest in topically applied products to reverse or delay the visible signs of photoaging. We discuss the most common topically applied agents for photoaging, reviewing their mechanisms and supporting evidence.
Key points
- •
Photoaging can be minimized or delayed with proper use of sun protection.
- •
Retinoids can reverse some of the signs of aging when used consistently.
- •
Vitamins applied topically can minimize damage from sun exposure and also act as antioxidants to limit environmental damage.
- •
The SPF system may underestimate the deleterious effects on the skin by neglecting the contributions of ultraviolet A radiation.
- •
Human studies of topically applied antioxidants are limited, but early work suggests they may have a protective effect against cellular changes resulting from photodamage.
Aging skin is among the most common patient concerns in a facial plastic surgery practice. Ultraviolet (UV)-induced damage expedites the pace of intrinsic aging, resulting in many of the visible signs of aging, such as rough skin texture, pigmentation irregularities, fine and deep wrinkling, and inelasticity. Primary prevention of UV and environmental damage with proper skin care and the use of sunscreen are critical. There is great interest in topically applied products to reverse or delay the visible signs of photoaging. There is an extraordinarily diverse array of prescription and cosmeceutical products available for the consumer. This article discusses the most common topically applied agents for photoaging, reviewing their mechanisms and supporting evidence.
Sunscreen
UV irradiation leads to the production of reactive oxygen species and activation of intracellular signaling pathways that result in an increase in inflammatory mediators. These mediators interfere with synthesis of dermal collagens and trigger synthesis of enzymes that degrade the extracellular matrix. This effect is compounded by UV damage to the mitochondrial genome, resulting in double-stranded breaks that affect the mitochondrial ability to produce energy for the cell and lead to further accumulation of reactive oxygen species. Moreover, chronic UV irradiation modifies local immunoregulation and cell survival, leading to impairment of intrinsic cancer surveillance. Both UVA and UVB spectrums are implicated in photodamage. UVB photons are on average 1000 times more energetic than UVA photons, making them a major contributor to photoaging and photocarcinogenesis. However, UVA is found in up to 10 times greater abundance in sunlight, and has greater depth of penetration into the dermis compared with UVB, giving it a possibly even greater role in photoaging. The visible effects of chronic long-term UV exposure are well-understood. The facial skin of females living in regions exposed to higher UV had significantly more and longer wrinkles, more and larger hyperpigmented spots, rougher surface texture, and more yellow discoloration based on computer analysis than women living at lower UV levels. Topical application of photoprotective agents significantly reduces the lifetime UV exposure compared with nonuse, with regular daily use beginning early in life being the most important factor. A randomized, controlled Australian study of 903 adults investigated the effect of daily use of a broad-spectrum sunscreen versus discretionary use and found that daily sunscreen use reduces the signs of skin aging based on skin surface replicas (level I evidence). Skin surface replicas were made from the back of the left hand by using a silicone-based impression material. These replicas were then graded by experienced evaluators who were blinded to their treatment group, and assessed based on severity of skin changes. This study found good intragrader and intergrader reliability.
There are 2 main categories of topically applied sunscreens: organic (previously called chemical) and inorganic (previously called physical). Organic sunscreens absorb UV irradiation, converting it to heat and thereby preventing its untoward effects in the skin. These compounds are typically not visible when applied and are therefore widely used. In contrast, inorganic sunscreens contain particles such as zinc oxide or titanium dioxide that reflect photons away from the skin. The earlier generations of inorganic sunscreens were less cosmetically desirable because their large particle size resulted in a visible and comedogenic coating on the skin. Newer iterations have micronized or nanosized the active particles, resulting in improved cosmetic appearance and alteration of the spectral absorption profile. The protection provided by sunscreen agents is traditionally quantified by SPF, or sun protection factor. This measure is defined as the minimal erythemal dose in sunscreen-protected skin divided by the minimal erythemal dose in non–sunscreen-protected skin. As UVB is the overwhelmingly greater contributing factor to sunburn than UVA, the SPF system was created to indicate the level of UVB protection. Thus, there is concern that the SPF system may underestimate the deleterious effects on the skin by neglecting the contributions of UVA radiation. Furthermore, the use of skin erythema as a surrogate for the more important underlying cellular alterations and local immunomodulation is called into question.
New awareness of the effects of UVA and its underrepresentation in current labeling systems prompted the US Food and Drug Administration (FDA) in 2011 to publish new guidelines directing the labeling and effectiveness testing for sunscreens. This ruling outlined the testing standards for coverage against both UVA and UVB for sunscreen to carry a label of “broad spectrum.” Also, this ruling for the first time provided permission for broad-spectrum sunscreen with SPF of 15 or greater to carry the claim to decrease skin cancer and early skin aging. One important issue addressed in the recent ruling is that there is no maximum allowable SPF label. Companies market sunscreens with SPF exceeding 100, which may provide consumers with a false sense of protection, resulting in prolonged UV exposure and failure to reapply sunscreen as directed. There is thus a recommendation by the FDA to cap the maximum SPF label at 50+, because there is not sufficient evidence to support increasing efficacy beyond SPF 50. There is not currently a UVA rating system in the United States, although a 5-star UVA protection rating system has been recommended for industry use in the European Union.
Sunscreen
UV irradiation leads to the production of reactive oxygen species and activation of intracellular signaling pathways that result in an increase in inflammatory mediators. These mediators interfere with synthesis of dermal collagens and trigger synthesis of enzymes that degrade the extracellular matrix. This effect is compounded by UV damage to the mitochondrial genome, resulting in double-stranded breaks that affect the mitochondrial ability to produce energy for the cell and lead to further accumulation of reactive oxygen species. Moreover, chronic UV irradiation modifies local immunoregulation and cell survival, leading to impairment of intrinsic cancer surveillance. Both UVA and UVB spectrums are implicated in photodamage. UVB photons are on average 1000 times more energetic than UVA photons, making them a major contributor to photoaging and photocarcinogenesis. However, UVA is found in up to 10 times greater abundance in sunlight, and has greater depth of penetration into the dermis compared with UVB, giving it a possibly even greater role in photoaging. The visible effects of chronic long-term UV exposure are well-understood. The facial skin of females living in regions exposed to higher UV had significantly more and longer wrinkles, more and larger hyperpigmented spots, rougher surface texture, and more yellow discoloration based on computer analysis than women living at lower UV levels. Topical application of photoprotective agents significantly reduces the lifetime UV exposure compared with nonuse, with regular daily use beginning early in life being the most important factor. A randomized, controlled Australian study of 903 adults investigated the effect of daily use of a broad-spectrum sunscreen versus discretionary use and found that daily sunscreen use reduces the signs of skin aging based on skin surface replicas (level I evidence). Skin surface replicas were made from the back of the left hand by using a silicone-based impression material. These replicas were then graded by experienced evaluators who were blinded to their treatment group, and assessed based on severity of skin changes. This study found good intragrader and intergrader reliability.
There are 2 main categories of topically applied sunscreens: organic (previously called chemical) and inorganic (previously called physical). Organic sunscreens absorb UV irradiation, converting it to heat and thereby preventing its untoward effects in the skin. These compounds are typically not visible when applied and are therefore widely used. In contrast, inorganic sunscreens contain particles such as zinc oxide or titanium dioxide that reflect photons away from the skin. The earlier generations of inorganic sunscreens were less cosmetically desirable because their large particle size resulted in a visible and comedogenic coating on the skin. Newer iterations have micronized or nanosized the active particles, resulting in improved cosmetic appearance and alteration of the spectral absorption profile. The protection provided by sunscreen agents is traditionally quantified by SPF, or sun protection factor. This measure is defined as the minimal erythemal dose in sunscreen-protected skin divided by the minimal erythemal dose in non–sunscreen-protected skin. As UVB is the overwhelmingly greater contributing factor to sunburn than UVA, the SPF system was created to indicate the level of UVB protection. Thus, there is concern that the SPF system may underestimate the deleterious effects on the skin by neglecting the contributions of UVA radiation. Furthermore, the use of skin erythema as a surrogate for the more important underlying cellular alterations and local immunomodulation is called into question.
New awareness of the effects of UVA and its underrepresentation in current labeling systems prompted the US Food and Drug Administration (FDA) in 2011 to publish new guidelines directing the labeling and effectiveness testing for sunscreens. This ruling outlined the testing standards for coverage against both UVA and UVB for sunscreen to carry a label of “broad spectrum.” Also, this ruling for the first time provided permission for broad-spectrum sunscreen with SPF of 15 or greater to carry the claim to decrease skin cancer and early skin aging. One important issue addressed in the recent ruling is that there is no maximum allowable SPF label. Companies market sunscreens with SPF exceeding 100, which may provide consumers with a false sense of protection, resulting in prolonged UV exposure and failure to reapply sunscreen as directed. There is thus a recommendation by the FDA to cap the maximum SPF label at 50+, because there is not sufficient evidence to support increasing efficacy beyond SPF 50. There is not currently a UVA rating system in the United States, although a 5-star UVA protection rating system has been recommended for industry use in the European Union.
Retinoids
Topical retinoids as a treatment for photoaging have the most extensive evidence-based support in the literature and, not surprisingly, has been widely adopted in clinical practice. Available topical retinoids include retinol, retinaldehyde, tretinoin (retinoic acid), isotretinoin, tazarotene, and adapalene. Tazarotene and adapalene are synthetic retinoinds.
Photodamage expedites the natural aging process resulting in skin discoloration, roughness, and wrinkles, the appearance of which can be improved with the use of retinoids. Retinoids act via a tretinoin-specific gene transcription factor, suggesting that retinoids leverage their effect on the skin through regulated gene expression. On a molecular level, retinoids bind to specific retinoic acid receptors, which serve as ligand-dependent transcription factors that regulate a diverse array of mediators to increase epidermal integrity and modulate the production of procollagen. As reviewed by Fisher and Voorhees in 1996, retinoid acts in vivo by inducing keratinocyte proliferation and modulating their differentiation, thereby increasing epidermal thickness, even by as much as 40% in some studies (compared with 10% in controls). This effect occurs regardless of topical or oral administration, which argues against a previously held belief that retinoid effect was mitigated solely through its irritant effect on the skin. Histologically, topical tretinoin has been shown to result in epidermal hyperplasia, compaction of the stratum corneum, and restoration of cell polarity. In addition to modulating cellular proliferation, some of the effects of retinoids may be mediated through collagen synthesis. Dermal collagen is central for providing resiliency to the skin, and its regulation and synthesis is an important component in the mechanism of the effect of tretinoin on photoaging. In a study by Talwar and colleagues, photoaged forearm skin was significantly lower in types I and III collagen compared with sun-protected underarm and buttock skin in a dose-dependent manner. A follow-up study demonstrated that 10 to 12 months of tretinoin use for photoaging resulted in a restoration of collagen I staining by 80% above baseline, compared with a 14% reduction in the control group.
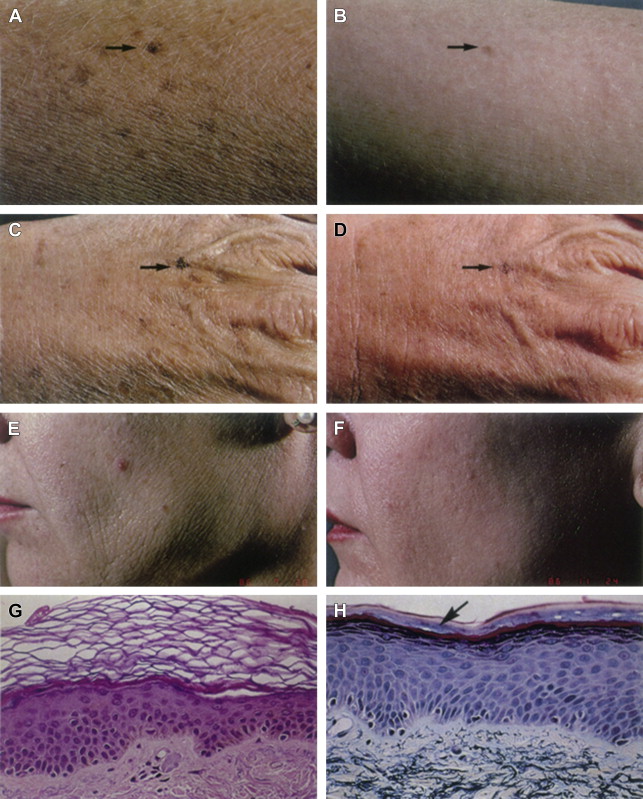
Early studies provided immediate promise for the use of retinoids. In a randomized, double-blind, placebo-controlled study from 1988, Weiss and colleagues enrolled 30 participants for a 16-week study during which 0.1% tretinoin was applied to 1 forearm, and a vehicle cream that did not contain tretinoin was applied to the other (level II evidence; only a single rater was utilized). One-half of the patients applied tretinoin to the face and the other half vehicle alone. Improvement in photoaging was reported in all of the treated forearms and in 14 of 15 patients who used tretinoin on the face, based on expert grading of fine and course wrinkling, tactile roughness, and telangiectasia. All parameters except telangiectasia showed improvement, and there was a reduction in the color of solar-induced freckles and lentigines, although not in the absolute lesion number. Skin biopsy specimens were also taken from the forearm, and demonstrated an increase in epidermal thickness and number of mitotic figures as well as an improved organization of the stratum corneum in the tretinoin treated group. This study also correlated clinical changes with histologic outcomes, and noted a significant increase in epidermal thickness and granular layer thickness, a higher mitotic index, and a compaction of the stratum corneum in the treated skin versus vehicle alone ( Fig. 1 ).
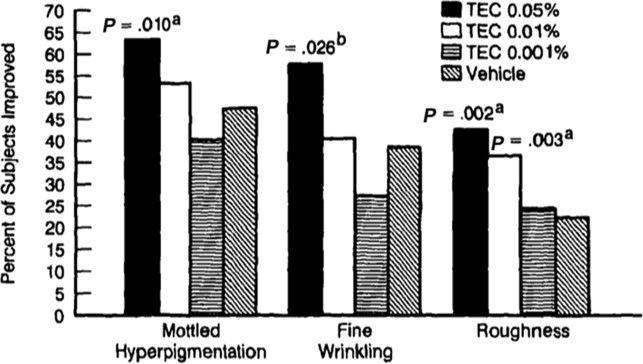
Small, early studies such as this were soon reinforced by larger multicenter trials, which have formed a strong evidence base for the efficacy of retinoic acid. A study of 251 patients compared topical tretinoin at concentrations of 0.05% and 0.01% versus vehicle control with outcome measure being improvement in photoaging based on a defined 9-point severity scale and histologic features on punch biopsy (level I evidence). This study demonstrated a significant improvement in photoaging score in the 0.05% group, which was supported by histologic changes, including increased epidermal thickness, decreased melanin content, and stratum corneum compaction. Notable side effects included erythema, peeling, burning, and stinging, which were more notable in the group treated with the higher concentration. A follow-up study from 1992 focused on the dose-related efficacy in comparing topical tretinoin at 0.05%, 0.01%, and 0.001% versus vehicle alone in a multicenter study of 296 patients (level I evidence). This study demonstrated that use of tretinoin 0.05% resulted in an improvement in overall severity of photodamage that increased with duration of use from 12 to 24 weeks, whereas 0.01% and 0.001% tretinoin were not different from vehicle alone in overall skin improvement ( Figs. 2 and 3 ). Recently, a 2-year, multicenter, double-blind, placebo-controlled trial of topical tretinoin 0.05% versus vehicle demonstrated the long-term efficacy of topical retinoic acid use, citing a significant improvement in fine and course wrinkling, mottled hyperpigmentation, and sallowness (level I evidence).