Chapter 2 Skin Care Including Chemical Peeling
Summary
Introduction
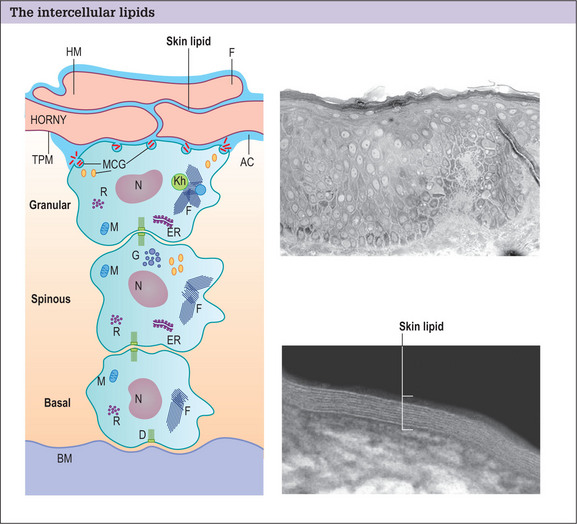
The skin is composed of three layers: the stratum corneum, epidermis, and dermis.
The stratum corneum forms the skin barrier and is composed of two distinct anatomic units:
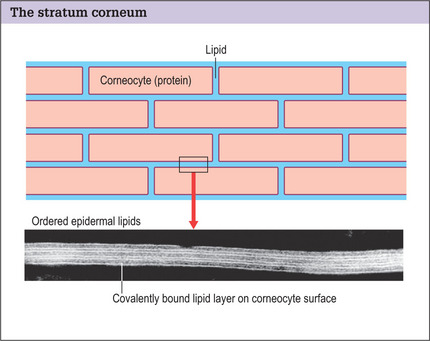
Structural damage to the corneocytes or to the lipids results in a defective barrier. With the aid of an electron microscope, it is possible to see the covalently bound lipid layer between the corneocytes forming an organized watertight seal over the body (Fig. 2.2).
Indications
Skin peeling is a controlled removal and renewal of the various layers of the skin, depending on the depth of the wound:
A chemical peel can be performed for a variety of indications:
Operative Approach
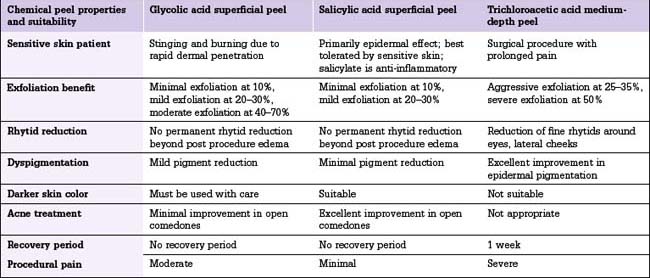
The peeling procedure for superficial, medium, and deep peels is somewhat similar, each deeper peel building on a more superficial skin wounding (Table 2.1).
Superficial peels
Glycolic acid peels
Glycolic acid peels in concentrations of 10% or less may be applied by unsupervised aestheticians in a spa setting, but concentrations of 20% or higher should be applied by a physician or in a carefully supervised setting.




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


