Fig. 15.1
The ViaDor™ Transdermal delivery system composed of the ViaDor™ device, disposable electrode array, and a suitable patch
The artificial skin pores formed by RF ablation, and their healing process, can be clearly seen by histological studies (Fig. 15.2). Application of the ViaDor™ device to pig’s skin appears to be minimally invasive and of a transient nature. The micropores crossed the stratum corneum and the entire epidermis and penetrated the papillary dermis. The histological findings demonstrate that healing takes place immediately after the MCs formation and that the healing process of the epidermis is gradual, as can be seen in Fig. 15.2. In a time window of 24 h, almost complete and natural recovery was observed. This gradual recovery process of the pores was also expressed by a gradual and constant decrease in delivery flux rate during 24 h, as expressed by in vitro and in vivo studies (Kam et al. 2012)
Fig. 15.2
Skin histology pictures
15.3 Thermal Ablation
Several systems for making pores using thermal ablation in the skin were reported. A transdermal delivery system, named PassPort®, was developed by Altea Therapeutics, and its know-how was acquired by Nitto Denko (Japan) on April 2012. This device is based on application of an array of metallic filaments (a “porator”) on the skin. Pressing the activation button of the applicator releases a single pulse of electrical energy to the porator, where the filaments convert the electrical energy into thermal energy. Rapid conduction of this thermal energy into tiny areas of the surface of the skin ablates the stratum corneum under each filament to create tiny pores of up to 50 micron in depth that just impinge into the viable epidermis. These microchannels are filled with interstitial fluid through which water-soluble molecules permeate to reach the viable tissues of the skin. From there, molecules can have either local effect or, by entering the circulation via the microcapillaries or lymphatic system, systemic effect (Smith and Tomlinson 2008).
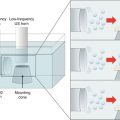
A different thermal skin ablation system, based on steam jet, was described. The device rapidly converts electrical energy into thermal and mechanical energy by ejecting a jet of superheated steam at the skin on a timescale on the order of 100 μs. This is done by capacitively discharging electric current directly through a few microliters of water in a microchamber. This permits extremely rapid and efficient heat transfer to the skin upon ejection from the device. It is claimed that this system may be inexpensive enough to be a onetime use, disposable device (Lee et al. 2011).
15.4 Laser Ablation
Laser skin microporation system was developed by Pantec Biosolutions (Germany). The P.L.E.A.S.E® (Painless Laser Epidermal System) device uses Er:Yag laser that emits light at 294 nm, which is the principle absorption wavelength for water molecules. Excitation of these molecules at specific points in the epidermis leads to heat generation, evaporation, and formation of pores (Bachhav et al. 2010). This technology was incorporated into two types of devices: P.L.E.A.S.E.® Professional for office or clinic use in conventional or aesthetic dermatology and P.L.E.A.S.E.® Private which is in development as a home device for use in combination with patch technologies for large molecule drug delivery.
It was found that laser treatment led to formation of cylindrical pores with diameters ranging from 150 to 200 μm. Pore depth was controlled by modification of the fluence (laser energy), and selective ablation of the stratum corneum was achieved by applying lower energies. The depth can be as low as 10–30 μm, which results in partially removal of the stratum corneum. The depth can also reach the epidermis at 50–80 μm or the dermis at 100–195 μm (Bachhav et al. 2010).
The laser ablation technology was shown to increase drug delivery flux through the skin. For drugs such as lidocaine (Bachhav et al. 2010) and prednisone (Yu et al. 2010), delivery rates in vitro were shown to increase significantly as a result of laser ablation treatment of the skin prior to drug application, either as an aqueous solution or as a cream.
15.5 Characterization of Skin Artificial Pores for Drug Delivery
Numerous studies demonstrated that transdermal delivery through the skin micropores created by ablation have unique characteristics compared to the regular transdermal delivery through intact skin:
Chemical nature of the delivered drugs – Unlike regular transdermal delivery, in which lipophilic molecules with log P of 1–3 are delivered most efficiently, the systemic transdermal delivery through ablation pores favors highly water-soluble drugs. Sintov et al. (2003) used a skin RF-ablation device to demonstrate in vitro and in vivo the significant delivery rate of the highly water-soluble granisetron hydrochloride compared to the sparingly water-soluble diclofenac sodium. It should be noted that the water-soluble salt of granisetron was used in this study, and not the more hydrophobic base version of the drug, that is more suitable for delivery through intact skin, as is used in the granisetron passive transdermal patch Sancuso (ProStrakan, Japan). Similarly, the water-soluble fentanyl citrate, and not the base form, was used for the development of fentanyl transdermal delivery system based on thermal ablation by the PassPort® device (Smith and Tomlinson 2008). Lee et al. (2011) used a different type of thermal skin ablation system to show a significantly increased transdermal flux of the hydrophilic fluorescent compounds sulforhodamine and Texas Red-labeled bovine serum albumin.
Molecular size – Applying RF-ablation device to the skin enables intradermal and transdermal penetration of large molecular size entities. Kim et al. (2012) showed that the in vitro delivery of FITC-dextran molecules as large as 40KD is enabled by forming pores in the skin using RF-ablation device. In the same paper, the delivery of epidermal growth factor (MW 6KD) through hairless mouse skin was demonstrated. Moreover, Levin et al. (2005) showed the delivery of human growth hormone (hGH, MW 22KD) through rat or guinea pig skin treated by a microporation device based on RF ablation. Insulin systemic transdermal delivery using thermal ablation (Smith and Tomlinson 2008) or RF ablation (Levin 2008) was demonstrated in several clinical trials. Other peptides and protein tested in vivo were interferon alpha-2b (Badkar et al. 2007) delivery by thermal ablation, salmon calcitonin, and human parathyroid hormone delivery by RF ablation (Stern and Levin 2012; Levin 2008; Nakano et al. 2011) as well as follicle-stimulating hormone transdermal delivery using laser ablation (Zech et al. 2011).
Bioavailability – The RF-ablation technology not only enabled the delivery of high molecular weight proteins but also permitted a very efficient transdermal delivery of protein drugs. Low bioavailability, as compared to parenteral administration methods, is one of the major obstacles for the development of user-friendly delivery methods for peptides and proteins. This low bioavailability significantly reduces the feasibility of developing these alternative delivery methods as commercial products. If the bioavailability of the protein using the delivery method is low (less than 10–20 %), there is a significant loss of protein resulting in higher manufacturing costs. This is despite the fact that more convenient delivery methods may probably increase patient compliance and therefore drug efficacy. The transdermal bioavailability of hGH relative to subcutaneous injection was found to be surprisingly high (75 % in rats and 33 % in guinea pigs) in a previous study (Levin et al. 2005). Moreover, even in human clinical trials, extremely high bioavailability results were found for systemic administration of peptides and proteins by transdermal delivery using RF-ablation technology. For example, the transdermal delivery of parathyroid hormone (PTH) showed a bioavailability of 40 % compared to subcutaneous injection (Levin 2008).
Dose response – It is well known that the stratum corneum functions as a rate controlling membrane in the case of regular transdermal delivery. Thus, increasing the dose of a drug on a fixed area patch doesn’t increase the dose delivered into the body. In order to increase the delivered dose of a regular transdermal product, the patch size is increased accordingly. In the case of transdermal delivery through the skin following RF-ablation device, it is possible to change the delivered dose through the same skin area by changing the patch dose. Levin et al. (2005) demonstrated a clear increase in the area under the plasma concentration curve (AUC) in response to increasing amounts of hGH in the patch. This dose response was linear within the dose range of 50–300 μg per 1.4 cm2 and was observed in both rats and GPs.Related posts:
 Iontophoresis: Basic Principles
Iontophoresis: Basic Principles
 Combined Use of Ultrasound and Other Physical Methods of Skin Penetration Enhancement
Combined Use of Ultrasound and Other Physical Methods of Skin Penetration Enhancement
 Transdermal Delivery of Peptides and Proteins by Physical Methods
Transdermal Delivery of Peptides and Proteins by Physical Methods
 Skin Vaccination Methods: Gene Gun, Jet Injector, Tattoo Vaccine, and Microneedle
Skin Vaccination Methods: Gene Gun, Jet Injector, Tattoo Vaccine, and Microneedle
 Electroporation for Dermal and Transdermal Drug Delivery
Electroporation for Dermal and Transdermal Drug Delivery
 Therapeutic Applications of Electroporation
Therapeutic Applications of Electroporation

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


