CHAPTER 15 Setting Up a Sclerotherapy Practice
Providers
Before proceeding with the practical aspects of establishing a practice, one must decide who will deliver patient care. Most physicians agree that a physician should perform the sclerotherapy procedure; however, some clinics use nurses to treat spider telangiectasias. A survey of the membership of the North American Society of Phlebology (NASP) (now the American College of Phlebology (ACP)) found that approximately 25% of the members would allow a registered nurse and 20% would allow a nurse practitioner to perform sclerotherapy on spider veins.1 Of NASP members surveyed, 10% would allow a registered nurse to perform sclerotherapy on varicose veins versus 7% who would allow nurse practitioners to perform this procedure. Registered nurses can legally perform intravenous therapeutic injections in most states. Physicians should check with the state licensing board for nursing for the specific requirements.
Because the cannulation of a blood vessel is relatively easy to perform and few serious or life-threatening complications can arise from sclerotherapy treatment of spider telangiectasias, an argument can be made for using nonphysicians as sclerotherapists. On the other hand, although rare, serious complications can result from injection of spider telangiectasias. Anaphylactic allergic reactions have occurred with many sclerosing agents; a fatality was reported after a ‘trial’ injection of sodium tetradecyl sulfate.2 Pulmonary emboli also have occurred from the injection of leg telangiectasias (see Chapter 8). Injection into an arteriovenous anastomosis usually produces a cutaneous ulceration, and cutaneous ulceration from sclerotherapy injection (extravasation or arteriolar injection) is the most common reason (in sclerotherapy) for medical malpractice litigation. Injection into a superficial artery, especially around the malleoli, can lead to arterial emboli and pedal gangrene. Duplex-guided injections into deep perforating veins can cause significant muscular necrosis requiring leg amputation. Thus, as with most of medicine, sclerotherapy is not entirely risk-free. The physician is ultimately responsible for ensuring that the nurse is properly trained both in performing sclerotherapy and in recognizing adverse sequelae. The physician, not the nurse, will be the one sued for malpractice.
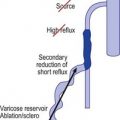
In addition to being skilled at sclerotherapy technique, the sclerotherapist must have a thorough knowledge of the anatomy and pathophysiology of venous disease and of the mechanism of action of the procedure, including its potential complications. The ability to appreciate these mechanisms and immediately recognize potential complications and render preventive treatment is critical to maintaining optimal patient care. Furthermore, a thorough understanding of vascular hemodynamics, including the relationship between deep and superficial venous insufficiency, is imperative to those practicing sclerotherapy. For example, venous segments with a certain degree of incompetence are best initially treated with endovenous ablation, which removes the source of venous hypertension, thus reducing or eliminating progression of reflux to other surrounding veins.3,4 Not being trained to recognize when endovenous ablation is a necessary portion of the overall treatment approach results in inadequate improvement following sclerotherapy. Thus, clinical judgment as well as technical skill are both essential attributes in an effective sclerotherapist.
Hallgren et al5 defined basic nursing assessment skills and the requirements for transfer of function of the nurse in a sclerotherapy–phlebology practice. In short, for a nurse to function as a sclerotherapist, the following must be known:
This knowledge base should also include instruction so that the nurse can do the following:
In conclusion, nurses who practice phlebology must be actively involved in the practice of nursing when delivering care. They should be able to prepare not only the operating room for the procedure, but also the patient for the procedure by answering questions, allaying fears, and documenting pretreatment disease. In addition, follow-up treatments allow the nurse the opportunity to reinforce patient teaching so that preventive measures can be emphasized. For an excellent demonstration of lower extremity superficial venous examination techniques, the reader is encouraged to refer to an educational DVD provided by the American College of Phlebology partnered with the Society of Vascular Ultrasound.6 Various other comprehensive textbooks on sclerotherapy, phlebectomy, and venous ultrasound techniques are available; we have referenced those textbooks that we feel are the most useful at the end of this chapter.7–10
Facility
Endovenous laser ablation of leg veins is best performed in a non-facility setting, as this eliminates additional facility fees associated with procedures performed in a hospital or ambulatory care facility. By having his/her procedure performed in an outpatient setting, patients save money by not having to pay facility fees, and practitioners generate more revenue by not having to split reimbursement payments with a facility.11
Equipment
Relatively little specialized equipment is required to perform successful sclerotherapy. Various types of lasers may also be required for treating specific types of leg veins (see Chapter 13). For now, all that is required is a needle, syringe, sclerosing solution, binocular loupe, foam pads, tape, graduated support stockings, and camera. ( See online Appendix C for information on manufacturers.) Although serious adverse events are rarely encountered during the treatment of leg veins, appropriate resuscitation equipment must be readily accessible throughout the procedure. Patients occasionally experience vasovagal reactions during the treatment of leg veins; ammonium capsules as well as oxygen can help mitigate these reactions. Other equipment, including an emergency resuscitation (crash) cart as well as an electrocardiograph, should remain readily accessible throughout the procedures.12
See online Appendix C for information on manufacturers.) Although serious adverse events are rarely encountered during the treatment of leg veins, appropriate resuscitation equipment must be readily accessible throughout the procedure. Patients occasionally experience vasovagal reactions during the treatment of leg veins; ammonium capsules as well as oxygen can help mitigate these reactions. Other equipment, including an emergency resuscitation (crash) cart as well as an electrocardiograph, should remain readily accessible throughout the procedures.12
Ultrasound devices
A duplex ultrasound device is essential for both diagnosis and treatment of venous disease. It can help discern superficial and deep venous insufficiency, allow for pretreatment vein mapping, provide imaging and guidance during the procedure, and allow for postoperative assessment of therapeutic efficacy.13
Needles
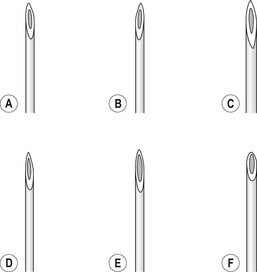
The injection of telangiectasias requires a fine-gauge needle. A needle with a clear plastic hub instead of a metal hub is useful to allow visualization with aspiration. Although some physicians prefer to use a 32- to 33-gauge or 26- to 27-gauge needle, we prefer the 30-gauge needle. There are two types of 30-gauge needles. One is the Becton-Dickinson (B-D) Precision Glide needle (Becton, Dickinson & Co, Rutherford, N.J.), which has an elongated bevel on a ½-inch needle with a 45-degree angle at the tip. The needle can be easily bent at varying angles to penetrate telangiectasias. In addition, it is relatively sharp and holds up well when used for multiple punctures of the skin. The second type is a tribevel tipped needle. The Acuderm (Acuderm, Ft Lauderdale, Fla.) and Delasco (Dermatologic Lab & Supply, Council Bluffs, Iowa) 30-gauge needles have a  -inch metal hub and a silicone-coated tribevel point. This type is preferred because its silicone coating and more acute angle at the tip allow it to pierce the skin with less pain. In addition, the length of the bevel is shorter than that of the B-D needle. Accordingly, extravasation of solution perivascularly while the needle is in the vessel lumen is less likely. Tribeveling of the tip also makes it harder, so it retains its sharpness with multiple injections. A comparison of the bevels of all of the recommended needles is shown in Figure 15.1. However, even with this magnified comparison, the differences between the needle tips cannot be fully appreciated. Clinical trials using each needle type are necessary to discern the subtle differences.
-inch metal hub and a silicone-coated tribevel point. This type is preferred because its silicone coating and more acute angle at the tip allow it to pierce the skin with less pain. In addition, the length of the bevel is shorter than that of the B-D needle. Accordingly, extravasation of solution perivascularly while the needle is in the vessel lumen is less likely. Tribeveling of the tip also makes it harder, so it retains its sharpness with multiple injections. A comparison of the bevels of all of the recommended needles is shown in Figure 15.1. However, even with this magnified comparison, the differences between the needle tips cannot be fully appreciated. Clinical trials using each needle type are necessary to discern the subtle differences.
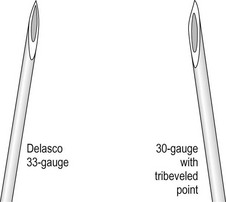
Some sclerotherapists advise the use of a 33-gauge needle to cannulate the smallest diameter telangiectasia. Multiple 31- to 33-gauge  -inch needles are available (Fig. 15.2). These needles have several drawbacks. They are more expensive than 30-gauge needles and must be cleaned and sterilized between patients if they are not disposed of (this is of concern to patients who fear inadequate sterilization with the subsequent risk of blood-borne pathogens). Repetitive sterilization also dulls the needle point. In addition, the tips of these needles bend and dull more quickly than those of the 30-gauge needles, and the needle shafts are thinner and thus less stable during injections through tough skin. John Phiffer (personal communication, 1992) reported on the construction of a rigid shaft used to support the 32-gauge needle tip to help stabilize it. However, as mentioned previously (Chapter 12), we find these needles of little use.
-inch needles are available (Fig. 15.2). These needles have several drawbacks. They are more expensive than 30-gauge needles and must be cleaned and sterilized between patients if they are not disposed of (this is of concern to patients who fear inadequate sterilization with the subsequent risk of blood-borne pathogens). Repetitive sterilization also dulls the needle point. In addition, the tips of these needles bend and dull more quickly than those of the 30-gauge needles, and the needle shafts are thinner and thus less stable during injections through tough skin. John Phiffer (personal communication, 1992) reported on the construction of a rigid shaft used to support the 32-gauge needle tip to help stabilize it. However, as mentioned previously (Chapter 12), we find these needles of little use.
 -inch length as either a Yale (Becton, Dickinson) hypodermic needle or as an allergy needle–syringe combination fixed to a 1-mm syringe. The benefit of using the 1-mm syringe is the ease of handling perceived by some sclerotherapists. The Yale 26-gauge needle also comes in a
-inch length as either a Yale (Becton, Dickinson) hypodermic needle or as an allergy needle–syringe combination fixed to a 1-mm syringe. The benefit of using the 1-mm syringe is the ease of handling perceived by some sclerotherapists. The Yale 26-gauge needle also comes in a  -inch length and has the advantage of a sturdy, nonbendable shaft. In short, all types have their advantages and disadvantages. The best needle is the one with which the physician is most comfortable.
-inch length and has the advantage of a sturdy, nonbendable shaft. In short, all types have their advantages and disadvantages. The best needle is the one with which the physician is most comfortable. inch, and the tubing is 30 cm. The plastic tubing on the proximal end of the needle allows visualization of arterial versus venous flow without risking blood exposure. The tubing takes up 0.41 mL of fluid. Some physicians fill the needle tubing with sclerosing solution to prevent clotting of blood within the needle tubing. However, this is unnecessary if the injection is performed within a few minutes of blood aspiration.
inch, and the tubing is 30 cm. The plastic tubing on the proximal end of the needle allows visualization of arterial versus venous flow without risking blood exposure. The tubing takes up 0.41 mL of fluid. Some physicians fill the needle tubing with sclerosing solution to prevent clotting of blood within the needle tubing. However, this is unnecessary if the injection is performed within a few minutes of blood aspiration. -inch needle on a short (
-inch needle on a short ( -inch) catheter tubing. The priming volume with this short length is 0.05 mL. The female Luer-Lok connector has a flange for easy grip. STD Pharmaceuticals (Hereford, UK) have a 30-gauge needle set with the needle attached to the tubing without wings and the other end of the tubing connected to a standard clear plastic female Luer-Lok [0].
-inch) catheter tubing. The priming volume with this short length is 0.05 mL. The female Luer-Lok connector has a flange for easy grip. STD Pharmaceuticals (Hereford, UK) have a 30-gauge needle set with the needle attached to the tubing without wings and the other end of the tubing connected to a standard clear plastic female Luer-Lok [0].Syringes
The 3-mL plastic syringe, Luer-Lok (Becton, Dickinson), is used exclusively in our practice. This syringe allows the use of an ideal quantity of solution, and when filled to a 2-mL capacity, it fits easily in the palm of the hand. However, a non-Luer-Lok syringe has the advantage of possessing a needle hub that is able to separate from the syringe if resistance, which indicates noncannulation of a vessel, is encountered. Each syringe manufacturer coats the inner portion of the syringe with silicone to allow smooth action by the plunger. The addition of silicone to coat the barrel of the syringe has also been shown to decrease the half-life of bubbles when foam is generated in the syringe (see Chapter 9). If using foam, one may wish to use a syringe with the least amount of silicone coating. The physician should evaluate different types of syringes to determine which has the best feel for his or her use.
If one does not bend the needle to facilitate penetration of the vein, the Plastipak eccentric syringe (Fig. 15.3) is useful. With this syringe, the hub is eccentrically placed at the syringe tip so that it abuts the skin surface. It is available in sizes of 1, 2, 5, and 10 mL.

Sclerosing solutions
The various sclerosing solutions available are discussed in detail in Chapter 7. Addresses of the manufacturers and distributors of these solutions are listed online in Appendix B .
.
Binocular loupes
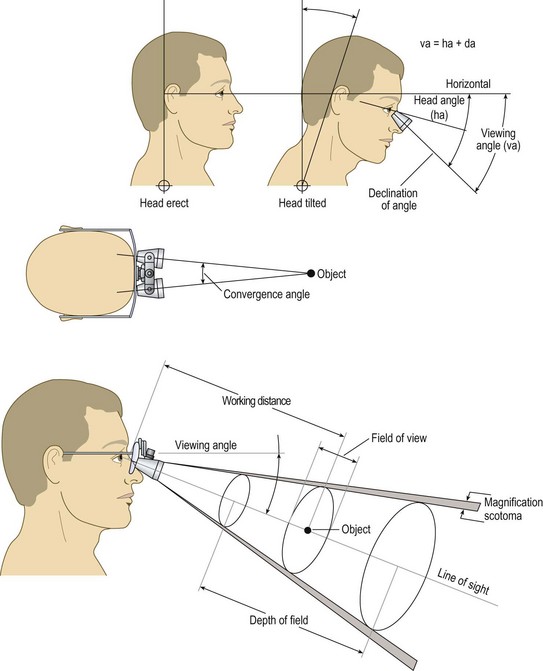
The ideal magnifier provides a wide field of view with distortion-free magnification within a reasonably long working distance and ergonomic viewing angle (Fig. 15.4). Unfortunately, with currently available optics, the higher the magnification, the smaller the field of view and depth of field. Complex, multilens binocular magnifiers overcome some of the limitations of short working distances. Some of these magnifiers are detailed online in Appendix C . An independent evaluation of magnifiers appears in another source.14,15
. An independent evaluation of magnifiers appears in another source.14,15
< div class='tao-gold-member'>




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


